This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
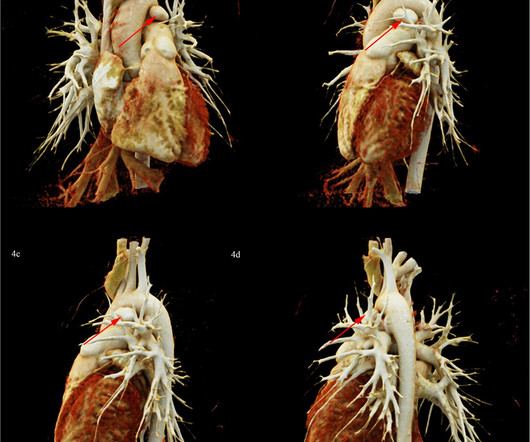
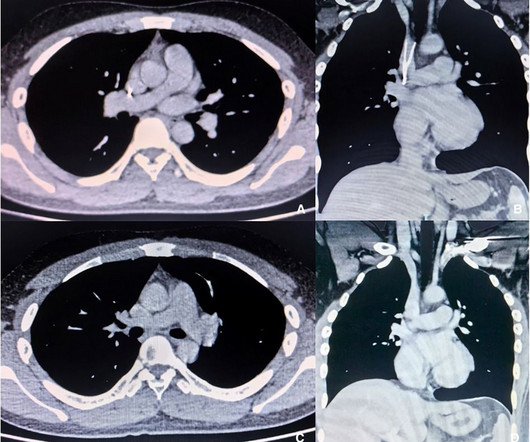
PDA combined with pulmonary artery aneurysm (PAA) due to IE is rare in children. Patent ductus arteriosus (PDA) is one of the most common forms of congenital heart disease (CHD). Infectious endocarditis (IE) is a rare but serious complication of PDA. In this report, we report a rare pediatric PDA case, complicated with PAA due to IE.
BACKGROUND:Aberrant BMPR2 (bone morphogenetic protein receptor 2) signaling is associated with the pathogenesis of pulmonary hypertension. By contrast, mice with smooth muscle cell-specificSmad4deletion had no pulmonary hypertension but rather displayed evident aortic aneurysm and dissection.
Idiopathic pulmonaryaneurysm is a clinically rare condition characterized by an unknown etiology and episodic occurrence. Despite its rarity, idiopathic pulmonary artery aneurysm poses potential risks to patients. Subsequently, she underwent surgical treatment.
To our knowledge, there have been extremely few clinical reports on coronary-pulmonary artery fistula (CPAF) accompanied by coronary artery aneurysm (CAA) and Vieussens arterial ring (VAR), and few reports on.
Ken (below) is appropriately worried about pulmonary embolism from the ECG. What I had not told him before he made that judgement is that the patient also had ultrasound B-lines of pulmonary edema. LV aneurysm has QS-waves, so this couldn't be LV aneurysm, right? What do you think? This is HIGHLY suspicious for OMI.
Patients with pulmonary atresia and ventricular septal defect (PA/VSD) are prone to progressive aortic dilation. However, there are relatively few reports of progressive development of aortic aneurysm or aorti.
He was in acute distress from pulmonary edema, with a BP of 180/110, pulse 110. He had diffuse crackles on exam and B-lines on chest ultrasound, and chest x-ray also confirmed pulmonary edema. The hypertension alone is the likely etiology of the pulmonary edema. He had no chest pain. The cath lab was activated.
Extra-pulmonary vein (PV) triggers have been reported in up to 4.9-15% 1,2 Eliminating identified extra-PV triggers is an important part of an AF ablation procedure after pulmonary vein isolation (PVI) is achieved.3 Extra-pulmonary vein (PV) triggers have been reported in up to 4.9-15%
Imaging revealed a large mass at the bifurcation of the main pulmonary artery, causing significant bil. A 9-day-old male neonate was found to have a systolic murmur during a routine follow-up for skin jaundice.
Pulmonary agenesis D. Ascending aortic aneurysm Answer: As the patient is a known case of arterial tortuosity syndrome, which is a rare hereditary disorder characterised by lengthening, dilatation and tortuosity of large and medium-sized arteries. The other images of the aneurysm are shown in. Left lung collapse C.
Preoperative ultrasonography and CT examination revealed that the filter retraction hook was very likely to penetrate the SVC wall and its tip was very close to the right pulmonary artery. The SVC was not obstructed, and no thrombus was observed in either upper limb.
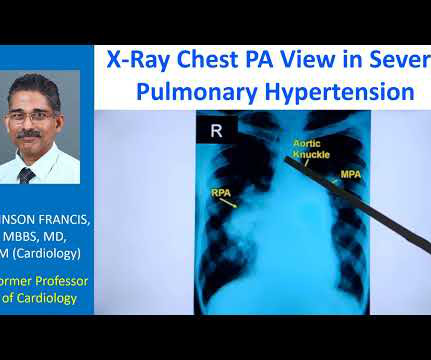
The striking finding is the huge enlargement of the right pulmonary artery, almost aneurysmal dilatation of right pulmonary artery. Main pulmonary artery is also grossly dilated. And you can see left pulmonary artery shadow and rest of it is not seen here. So massive enlargement of pulmonary arteries.
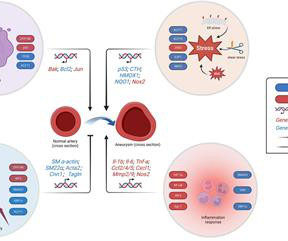
KLF11 prevents aneurysm progression by inhibiting the apoptosis of VSMCs and enhancing their contractile function. The Krüppel-like family (KLF) TF family is widely recognized as the foremost regulator of vascular diseases.
Smith : Old inferior MI with persistent ST Elevation ("inferior aneurysm") has well-formed Q-waves. In inferior aneurysm, we usually see QR-waves, whereas for anterior aneurysm, we see QS-waves (no R- or r-wave at all!). The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent.
There are two forms of HHT: (HHT1) has a higher incidence in women and typically involves pulmonary and cerebral arteriovenous malformations (AVM). Given the heavy cerebral AVM burden with multiple cerebral artery feeders, the AVM angiosclerosis and basilar artery aneurysm embolization were deferred.
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. I would do bedside ultrasound to look at the RV, look for B lines as a cause of hypoxia (which would support OMI, and argue against PE), and if any doubt persists, a rapid CT pulmonary angiogram.
Cardiovascular neurocristopathy, i.e., cardiopathy and vasculopathy, associated with the NCC could occur in the form of (1) cardiac septation disorders, mainly the aortico-pulmonary septum; (2) great vessels and vascular disorders; (3) myocardial dysfunction; and (4) a combination of all three phenotypes.
IntroductionSubarachnoid Hemorrhage (SAH) resulting from the spontaneous rupture of an aneurysm is a rare and highly debilitating condition. Despite its severity, patients with aneurysmal SAH remain understudied, particularly concerning the evaluation of the incidence and consequences of subsequent acute kidney injury (AKI).
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." The computerized interpretation for this tracing was, “Sinus rhythm; Normal ECG” — and attention of acute care providers was apparently focused on attending to this patient’s pulmonary problems.
The patient's heart had significant recovery: Echo : Estimated LVEF 32%, apical wall motion abnormality with diastolic distortion (LV aneurysm), suggestive of old MI. pulmonary embolism, sepsis, etc.), A followup ECG was recorded 2 days later: No definite evidence of infarction. It was uncertain whether this represented: 1.
By these mechanisms, SMC-MR promotes disease progression in models of aging-associated vascular stiffness, vascular calcification, mitral and aortic valve disease, pulmonary hypertension, and heart failure. While rarely tested, when sexes were compared, the mechanisms of SMC-MR-mediated disease were sexually dimorphic.
Pulmonary Arterial Hypertension (PAH): Hasan Ahmad Khasawneh’s (Jordan) systematic review of Treprostinil safety in PAH patients revealed no significant increase in mortality, though adverse events were more frequent. This debate underscored the growing role of CSP despite the current limited evidence supporting it.
CT angiogram chest: no aortic dissection or pulmonary embolism. Serial chest xrays: progressive bilateral pulmonary edema. Repeat CT angio chest (not CT coronary, unclear what protocol) showed possible LAD aneurysm and thrombus. No further troponins were measured. No further cath details available. This gets drilled into them.
Rupture can be either free wall rupture (causing tamonade) or septal rupture, causing ventricular septal defect with left to right flow and resulting pulmonary edema and shock. Additionally , these patients have a high incidence of LV aneurysm with mural thrombus. If detected early by ultrasound, the patient can be saved.
There are no Q-waves to suggest old inferior MI, or inferior aneurysm as the etiology of the ST Elevation. I suspect pulmonary edema, but we are not given information on presence of B-lines on bedside ultrasound, or CXR findings. Acute coronary occlusion and acute pulmonary edema can coexist. What other pathology is possible?
Look for Vascular Etiology -- think of these while doing H and P: --Bleeding: ruptured AAA, GI bleed, ruptured ectopic pregnancy, other spontaneous bleed such as mesenteric aneurysms. Serious outcomes included death, arrhythmia, myocardial infarction, structural heart disease, pulmonary embolism, and hemorrhage. of ED visits.
thoracic aortic dissection, thoracic aortic aneurysm, and/or type B intramural hematoma) as well as the presence of T1ELs or T2ELs.ResultsReoperation was more common in the T1EL group (n=4; 57%) than in the T2EL group (n=2; 29%); also, reintervention for stenting of the thoracic endovascular graft was more frequent in the T1EL group (4 vs. 1).
His initial high sensitivity troponin I returned at 1300 ng/L and given that his cardiac workup was otherwise unremarkable, a CT was obtained to evaluate for pulmonary embolism and aortic aneurysm or dissection but this too was unrevealing. Also: electrical instability, pulmonary edema, or hypotension.
When there are QS-waves, one should always think about LV aneurysm, but ST to QRS ratio and T-wave to QRS ratio are far too large and not compatible with left ventricular aneurysm. There is some R wave in the lateral precordial leads. Leads V3 and V4 both have 6mm ST elevation. This ECG shows a lot of "acuity".
No thoracic aortic hematoma, aneurysm or dissection. No pulmonary embolism is identified. While in the ED, patient's pain worsened to previous severity of 6/10 pain and improved to 3/10 on NTG drip. CT Angio Chest IMPRESSION 1. There are moderate coronary artery calcifications.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content