This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Kawasaki disease (KD), an acute self-limited febrile illness that primarily affects children <5 years old, is the leading cause of acquired heart disease in developed countries, with the potential of leading to coronary artery dilation and coronary artery aneurysms in 25% of untreated patients.
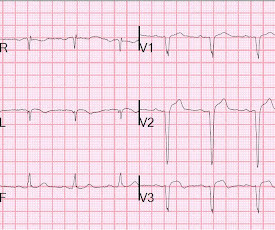
There are QS-waves in V1-V3 suggesting old anterior MI with persistent ST Elevation (LV aneurysm morphology), but I have written a couple papers showing that in LV aneurysm, the T-wave is not > 0.36 T/QRS Amplitude Best Distinguishes Acute Anterior MI from Anterior Left Ventricular Aneurysm. LV Aneurysm vs New Infarction?
The conventional algorithm said: SINUS RHYTHM ANTERIOR MYOCARDIALINFARCTION , PROBABLY RECENT [40+ ms Q WAVE AND/OR ST/T ABNORMALITY IN V3/V4] ACUTE MI There are well-formed Q-waves in precordial leads. The patient is pain free now, so it is either a reperfused subacute MI or a Non-OMI superimposed on an old MI (aneurysm).
We performed coronary angiography for the patient with ECMO support, indicating that the patient had an 80% critical stenosis of the left main coronary artery and an 80%–90% stenosis in the middle section of the left anterior descending artery with an aneurysm. Fortunately, there was no obvious stenosis in the right coronary artery.
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
STEMI – Anterior Wall ECG shows ST elevation myocardialinfarction of anterior wall. Up sloping elevation of ST segment is seen in leads V1 to V5, with maximum ST elevation in V2, as is characteristic of anterior wall infarction. QS complexes are seen from V1 to V3.
ECG changes resembling ST elevation myocardialinfarction has also been described after traumatic intracranial hemorrhage [4]. Excess of catecholamines can damage myocytes directly and can also lead to generalized spasm of coronary arteries and even consequent actual myocardialinfarction [5]. Images in clinical medicine.
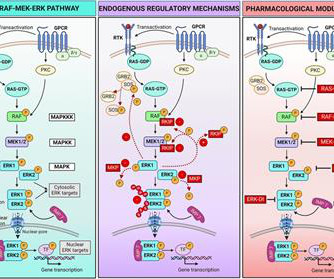
We then summarize current knowledge of the roles played by ERK in the development and progression of cardiac and vascular disorders, including atherosclerosis, myocardialinfarction, cardiac hypertrophy, heart failure, and aortic aneurysm.
This may resolve over a couple weeks; if it does not, then he is at high risk of developing an LV aneurysm, or diastolic dysfunction of the anterior wall. 4) Q-waves alone do not necessarily imply irreversibly infarcted myocardium; they should not dissuade from reperfusion therapy. He has persistent ST elevation. Raitt MH et al.
So this is indeed diagnostic of myocardialinfarction. Not immediately, at least, because this is NOT diagnostic of ACUTE (occlusion) myocardialinfarction (Acute OMI). To repeat: in contrast, anterior aneurysm is much more easily distinguished from acute MI due to the QS-waves. Should we activate the cath lab?
Persistent ST elevation 3 days after a nearly transmural MI portends possible LV aneurysm. Here there are some QS-waves, telling us that there has probably been a significant amount of completed infarction, but there is also persistent R-wave in lead V4 suggesting some viable myocardium. Zwolle MyocardialInfarction Study Group.
IntroductionSubarachnoid Hemorrhage (SAH) resulting from the spontaneous rupture of an aneurysm is a rare and highly debilitating condition. Despite its severity, patients with aneurysmal SAH remain understudied, particularly concerning the evaluation of the incidence and consequences of subsequent acute kidney injury (AKI).
Is LVH like left ventricular aneurysm? However, an analogous rule for identifying superimposed ACO of the LAD in the presence of persistent STE after prior MI (aka “ left ventricular aneurysm ,” or LVA) was just validated. ST elevation: differentiation between ST elevation myocardialinfarction and nonischemic ST elevation.
Alternatively , it is someone who has an old myocardialinfarction and is now very sick with something else. Old MI with persistent ST Elevation (LV aneurysm morphology) can look like acute MI 2. Not all anterior LV aneurysm has a QS-wave. LV Aneurysm? Below is my response. There is sinus tach. Learning Points: 1.
Case A 43 year old male with a history of DM II, hyperlipidemia, and a family history of myocardialinfarction presented to a family clinic with two days of epigastric pain that started after consuming a meal. The LV aneurysm morphology persists. Because: 1) He has been reading this blog for a long time.
This unique case highlights the diagnostic and therapeutic challenges of a patient with multiple vascular risk factors who suffered from strokes secondary to BHS.MethodsA 79‐year‐old man with a past medical history of peripheral artery disease, abdominal aortic aneurysm, myocardialinfarction with drug eluding stents (on dual antiplatelet therapy (DAPT)), (..)
Read our recent editorial: Hyperacute T-waves Can Be a Useful Sign of Occlusion MyocardialInfarction if Appropriately Defined. Relationship between an in-farct related artery, acute total coronary occlusion, and mortality in patients with ST-segment and non-ST-segment myocardialinfarction. hours earlier? Circulation.
Although not striking, this is clearly a diagnostic ECG for infero"posterior" myocardialinfarction due to coronary occlusion (OMI), most likely due to left circumflex (LCx) artery occlusion. mm STE even in the fourth universal definition of myocardialinfarction. Considerations on the naming of myocardialinfarctions.
A followup ECG was recorded 2 days later: No definite evidence of infarction. The patient's heart had significant recovery: Echo : Estimated LVEF 32%, apical wall motion abnormality with diastolic distortion (LV aneurysm), suggestive of old MI. MINOCA: MyocardialInfarction in the Absence of Obstructive Coronary Artery Disease).
Mid cavity obstruction in HCM is associated with apical aneurysm, systemic embolism, and arrhythmias. Thin posterior wall in inferior wall myocardialinfarction causing abnormal septal to posterior wall ratio can also cause suspicion of ASH. Doppler echo showing LVOT gradient in HCM.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Cardiac Troponin Changes to Distinguish Type 1 and Type 2 MyocardialInfarction and 180-Day Mortality Risk. You do NOT see this in normal variant STE, nor in pericarditis. Murakami M.
A CT was completed to rule out dissection, PE, or aneurysm, and this was unremarkable. Association between opioid analgesia and delays to cardiac catheterization of patients with occlusion MyocardialInfarctions. Clin Cardiol 2022; [link] Labs included: hsTnI 156 ng/L, Hb 12 g/dL, WBC 12x10^9/L, Cr. mg/dL, K 3.5 Abstract 556.
Repeat ECG at 1624 (shortly before cath): QS waves now present in V2-V3, with slight STE, showing the pattern of left ventricular aneurysm morphology. Next trop 85,528 ng/L (consistent with a massive myocardialinfarction), none further measured. Upon arrival to the PCI center, the repeat troponin returned at 13,962 ng/L.
Variables and prognosis were analysed based on the presence or absence of NCA, defined as previous stroke, transient ischaemic attack (TIA), or peripheral artery disease (PAD) [lower extremity artery disease (LEAD), carotid disease, previous lower limb vascular surgery, or abdominal aortic aneurysm (AAA)].
Additionally , these patients have a high incidence of LV aneurysm with mural thrombus. Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. Although rupture has a high mortality, it is not uniformly fatal References 1. Armstrong PW et al.
Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. Perhaps she will not develop an LV aneurysm. Myocardial Rupture and Postinfarction Pericarditis. The ECG in myocardial rupture 94. These do NOT indicate late, subacute MI.
The protein model also improved the prediction of other outcomes, including ASCVD (cstatistic +0.035), myocardialinfarction (+0.023), stroke (+0.024), aortic stenosis (+0.015), heart failure (+0.060), abdominal aortic aneurysm (+0.024), and dementia (+0.068).CONCLUSIONS:Measurement
1,2 ASCVD causes or contributes to conditions that include coronary artery disease (CAD), cerebrovascular disease, and peripheral vascular disease (inclusive of aortic aneurysm).3 Efficacy and Safety of Low-Dose Colchicine after MyocardialInfarction. 4 In the U.S. 35 Overall, the magnitudes of benefit seen from colchicine, 0.5
In most cases, rather, the culprit is gross ischemia due to myocardialinfarction, cardiomyopathy, or advanced coronary artery disease. It was postulated that such an ECG feature is associated with advanced myocardial dysfunction, to include left ventricular aneurysm, as the cause of arrhythmia. [7]
She went for a head CT and had a severe subarachnoid hemorrhage (SAH) due to ruptured aneurysm. Door to balloon time (DBT) was 96 minutes for 7 patients with ST elevation myocardialinfarctions (STEMI) who had CT prior to PCI vs. 75 minutes for 11 patients who did not have CT, p=0.058. Conclusions: Head CT is common in NT-OHCA.
You might think it is "Old MI with persistent ST Elevation" (otherwise known as "LV aneurysm" morphology.") That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. Formula value = 20.89, which is much higher than the cutpoint of 18.2
Look for Vascular Etiology -- think of these while doing H and P: --Bleeding: ruptured AAA, GI bleed, ruptured ectopic pregnancy, other spontaneous bleed such as mesenteric aneurysms. to 1.64) for myocardialinfarction or death from coronary heart disease, and 1.06 (95 percent confidence interval, 0.77 Left axis deviation, 5.
When there are QS-waves, one should always think about LV aneurysm, but ST to QRS ratio and T-wave to QRS ratio are far too large and not compatible with left ventricular aneurysm. It could also, given a different clinical context be compatible with a subacute myocardialinfarction complicated by post infarct regional pericarditis.
No thoracic aortic hematoma, aneurysm or dissection. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients. Patient states pain improved on ambulance ride over after receiving 325 mg Aspirin and nitroglycerin, with pain down to 2/10.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content