This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
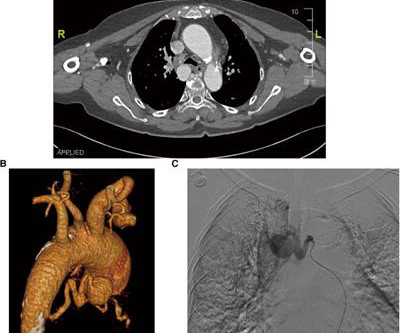
Bronchial artery aneurysm (BAA) is a rare and fatal condition that requires immediate treatment. In the present case, a 76-year-old hypertensive woman was admitted with dizziness and diagnosed with an unruptured bronchial artery aneurysm, which was treated by transcatheter arterial embolization and aortic stent-graft.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. The hypertension alone is the likely etiology of the pulmonary edema. He had no chest pain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
Clinical introduction The patient was a man in his 40s with a medical history of hypertension, Behcet’s disease (BD) and chronic renal dysfunction. The patient was receiving therapeutic doses of the following medications: sacubitril valsartan sodium tablets, prednisone acetate, cyclophosphamide and azathioprine.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. Does this change your interpretation?
She is somewhat hypertensive, but her vital signs are otherwise normal. However, old MI w/aneurysm morphology (persistent ST-Elevation) can look just like this. While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change.
Common comorbidities included hypertension (62.5%), smoking (56.3%), and hyperlipidemia (46.9%). Of the 32 patients, 9(28.1%) had dissection with diagnostic angiograms, 6(18.8%) endovascular thrombectomy, 15(46.9%) aneurysm treatment, and 2(6.3%) angioplasty with or without stenting. One patient was symptomatic with neck pain.
This unique case highlights the diagnostic and therapeutic challenges of a patient with multiple vascular risk factors who suffered from strokes secondary to BHS.MethodsA 79‐year‐old man with a past medical history of peripheral artery disease, abdominal aortic aneurysm, myocardial infarction with drug eluding stents (on dual antiplatelet therapy (DAPT)), (..)
Her vitals signs were remarkable for marked hypertension. All these factors, again, support an ECG diagnosis of LVH The patient was nonetheless taken for emergency angiography, and a 99% mid-LAD lesion was found and stented. Is LVH like left ventricular aneurysm? An ECG was obtained at triage: ECG #1 at 0000 hours.
New guidelines also: Classify “Elevated BP” between non-elevated BP and hypertension. Measuring eGFR and albuminuria is recommended for assessing kidney disease in all hypertensive patients. Advise increased potassium intake for hypertensive patients.
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chest pain that started while mowing the lawn. The LAD lesion was acute and required 3 stents to restore flow. Here is his ECG on arrival: What do you think?
He carries the diagnoses hyperlipidemia, hypertension, and diabetes. No thoracic aortic hematoma, aneurysm or dissection. First obtuse marginal also had an 80% stenosis and was stented. He presented to the ED for evaluation chest pain. Pain was improved but not gone upon arrival. CT Angio Chest IMPRESSION 1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content