This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
She is somewhat hypertensive, but her vital signs are otherwise normal. However, old MI w/aneurysm morphology (persistent ST-Elevation) can look just like this. While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change.
Common comorbidities included hypertension (62.5%), smoking (56.3%), and hyperlipidemia (46.9%). Of the 32 patients, 9(28.1%) had dissection with diagnostic angiograms, 6(18.8%) endovascular thrombectomy, 15(46.9%) aneurysm treatment, and 2(6.3%) angioplasty with or without stenting.
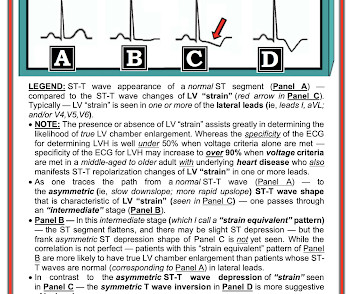
Her vitals signs were remarkable for marked hypertension. However, the ST segments in patients with LVH may show significant variation over time in the absence of ischemia. 3 Some have also suggested that the typically asymmetric T wave inversion (TWI) of LVH might be distinguished from the typically symmetric TWI of cardiac ischemia.
He was mildly tachycardic (105-110 bpm) and hypertensive (157/92 mm Hg) on arrival. Repeat ECG at 1624 (shortly before cath): QS waves now present in V2-V3, with slight STE, showing the pattern of left ventricular aneurysm morphology. Cardiologist interpretation: "Technically does not meet STEMI criteria but concerning for ischemia."
Background:According to the 2023 guidelines for the management of patients with aneurysmal subarachnoid hemorrhages (SAH), early treatment of ruptured aneurysms reduces the risk of repeated bleeds and facilitates treatment of delayed cerebral ischemia. No differences were noted in the size or location of aneurysm.
A middle-age woman with h/o hypertension was found down by her husband. This ECG is diagnostic of diffuse subendocardial ischemia. She went for a head CT and had a severe subarachnoid hemorrhage (SAH) due to ruptured aneurysm. Medics found her apneic and pulseless, began CPR, and she was found to be in asystole.
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chest pain that started while mowing the lawn. His chest pain was located in the central chest, non-radiating, and associated with diaphoresis, nausea, and vomiting.
iv ) The findings in Figure-4 could reflect LV aneurysm. C ASE F ollow- U p: I later learned the history in today's case which was that a middle-aged man with diabetes and hypertension who presented to the ED ( E mergency D epartment ) for abdominal pain that had awakened him from sleep. Radionuclide scan was negative for ischemia.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chest pain and shortness of breath. There are no Q-waves to suggest old inferior MI, or inferior aneurysm as the etiology of the ST Elevation. The patient was started on heparin for possible NSTEMI vs demand ischemia.
When there are QS-waves, one should always think about LV aneurysm, but ST to QRS ratio and T-wave to QRS ratio are far too large and not compatible with left ventricular aneurysm. There were no other causes of dyspnea apparent and thus we can assume that myocardial ischemia started 6 days prior.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content