This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
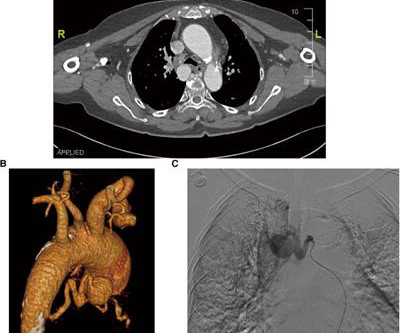
Bronchial artery aneurysm (BAA) is a rare and fatal condition that requires immediate treatment. However, conventional surgical and transcatheter arterial embolization treatments are less effective. Simultaneously, we reviewed 79 research papers, analyzing past BAA cases for their etiology, symptoms, and treatment outcomes.
Life‐threatening bleeds may occur from the AVM nidus or associated aneurysms. Two large inflow aneurysms, felt to be the rupture site, projecting from the proximal left pericallosal artery were also demonstrated. An incidental ACA aneurysm was also noted. Onyx‐18 was then injected into the main AVM pedicle under a blank roadmap.
IntroductionThe use of detachable coils for endovascular embolization of cerebral aneurysms has become a safe and effective alternative to direct surgical clipping in patients with ruptured aneurysmal subarachnoid hemorrhage. Immediate complete occlusion and occlusion with residual neck was achieved in 66.7%
IntroductionFlow diversion (FD) is commonly used for the treatment of aneurysms involving the ophthalmic segment of the carotid artery (COA). The origin of the ophthalmic artery (OA) in relation to the aneurysm sac can affect recurrence and complications. directly from the aneurysm fundus, B. aneurysm neck, C.
IntroductionInfectious intracranial aneurysms (IIAs), commonly referred to as mycotic aneurysms, are a common sequela of infective endocarditis (IE). were treated with an endovascular approach; 50% underwent onyx embolization, 28.6% underwent n‐BCA embolization, 14.2% Among those IIAs treated, 92.8% 9); (P=0.002).
IntroductionIntracranial aneurysms, both ruptured and unruptured, pose a significant risk to the general population. Cases of unruptured intracranial aneurysms (UIA) are estimated to affect roughly 3% of the general population and aneurysmal subarachnoid hemorrhage (aSAH) have an incidence of 8 to 9 people per 100,000.
IntroductionThe Pipeline Embolization Device (PED) is commonly used for intracranial aneurysm treatment. While its effectiveness for certain types of aneurysms is well‐established, its efficacy for saccular aneurysms remains debatable. Secondary outcomes included long‐term complications. The mean age was 55.7
IntroductionTo provide our single‐institution experience and outcome data with the WEB device in 51 patients treated for ruptured and unruptured intracranial aneurysms.MethodsOcclusion rates in a cohort of 51 patients treated with WEB were collected at time of procedure and at last follow‐up between the years 2019 and 2021.
IntroductionIndications for flow diversion for the treatment of cerebral aneurysms have increased remarkably in recent years.1 1 This has been particularly useful for aneurysms that are difficult to treat via endosaccular or open approaches, such as pseudoaneurysms.2
IntroductionBasilar‐tip aneurysm (BTA) is the most common aneurysm found in the posterior circulation, representing 5–8% of total intracranial aneurysms. Coil embolization (CE) is safer and more efficacious in the treatment of BTAs compared to open surgery but has increased rate of recanalization. vs. 10.7%).
Eventually, the PSA of the Internal maxillary artery (IMAX) was embolized, resulting in resolution of the patient's symptoms.MethodsCase ReportResultsA 75‐year‐old male with a history of atrial fibrillation on Eliquis presented to the emergency department after sustaining a gunshot wound to the left face.
IntroductionRuptured aneurysmal SAH accounts up to 80% of nontraumatic SAH, with more than 80% located in the anterior circulation and a mortality rate upwards of 50%.1‐3 1,2,4–6 Despite this, EVT of intracranial aneurysms has its own risk of complications including intraoperative rupture and thromboembolic events.7
This study aims to investigate the incidence, complications, and outcomes of SAH patients who develop HIT.MethodsICD‐9‐CM and ICD‐10‐CM codes were used to query the National Inpatient Sample for patients with SAH between 2010 and 2019. Patients with SAH are an understudied population in terms of assessing incidence and impact of HIT.
IntroductionSubarachnoid Hemorrhage (SAH) resulting from the spontaneous rupture of an aneurysm is a rare and highly debilitating condition. Despite its severity, patients with aneurysmal SAH remain understudied, particularly concerning the evaluation of the incidence and consequences of subsequent acute kidney injury (AKI).
CT angiogram chest: no aortic dissection or pulmonary embolism. Repeat CT angio chest (not CT coronary, unclear what protocol) showed possible LAD aneurysm and thrombus. Smith Major Learning Point: The worst risk factor for a bad outcome in OMI is young age because cardiologists cannot believe that a young person can have an OMI.
Both of these are very suggestive of " No-Reflow ," or poor microvascular reperfusion due to downstream embolization of microscopic platelet-fibrin aggregates. Perhaps she will not develop an LV aneurysm. A cutoff of 9 mm for inferior AMI and 13 mm for anterior AMI predicted worse outcome. That remains to be seen.
Look for Vascular Etiology -- think of these while doing H and P: --Bleeding: ruptured AAA, GI bleed, ruptured ectopic pregnancy, other spontaneous bleed such as mesenteric aneurysms. Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Abnormal ECG – looks for cardiac syncope.
No thoracic aortic hematoma, aneurysm or dissection. No pulmonary embolism is identified. A paradox in the literature: All trials of very early intervention for NSTEMI which do not exclude patients with persistent chest pain show that intervention in < 2 hours results in a better outcome. CT Angio Chest IMPRESSION 1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content