This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
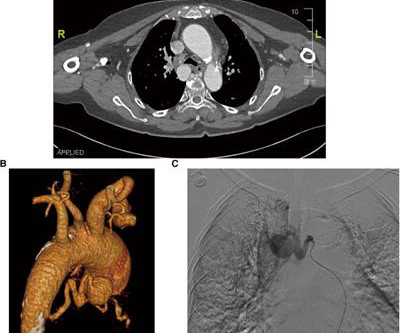
Bronchial artery aneurysm (BAA) is a rare and fatal condition that requires immediate treatment. However, conventional surgical and transcatheter arterial embolization treatments are less effective. The patient's clinical status was stable during the 4-year follow-up.
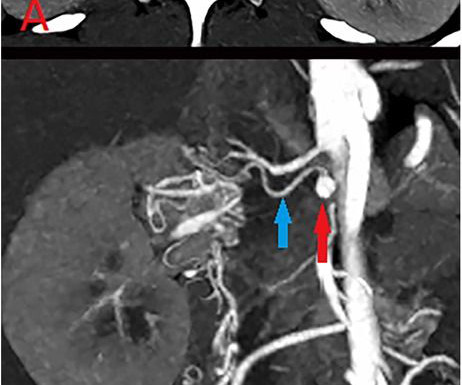
IntroductionThis study reports a patient who developed a secondary renal artery aneurysm (RAA) after occlusion of the main renal artery.MethodsA 25-year-old woman was hospitalized due to an enlarged renal artery aneurysm (RAA). The left kidney function remained normal, allowing successful aneurysmembolization.
IntroductionCerebral aneurysms are a rare cause of headaches and visual symptoms. While most unruptured aneurysms are asymptomatic, when symptoms do occur, they are most often headaches, cranial nerve palsies, or bilateral temporal hemianopsia due to compression of surrounding nerves or the optic chiasm.
Introduction18‐36% of all intracranial aneurysms are middle cerebral artery(MCA) bifurcation aneurysms. 1) MCA bifurcation aneurysms have been historically challenging to treat endovascularly given they often have complex morphology and wide necks. Final angiography revealed complete occlusion of the aneurysm.
Life‐threatening bleeds may occur from the AVM nidus or associated aneurysms. Two large inflow aneurysms, felt to be the rupture site, projecting from the proximal left pericallosal artery were also demonstrated. An incidental ACA aneurysm was also noted. Onyx‐18 was then injected into the main AVM pedicle under a blank roadmap.
Ken (below) is appropriately worried about pulmonary embolism from the ECG. LV aneurysm has QS-waves, so this couldn't be LV aneurysm, right? RBBB makes it mandatory that there are R'-waves even in the presence of LV aneurysm. Patients with anterior LV aneurysm usually have poor LV function and heart failure.
IntroductionIntracranial aneurysms, both ruptured and unruptured, pose a significant risk to the general population. Cases of unruptured intracranial aneurysms (UIA) are estimated to affect roughly 3% of the general population and aneurysmal subarachnoid hemorrhage (aSAH) have an incidence of 8 to 9 people per 100,000.
years) underwent surgery for unruptured anterior communicating artery aneurysms in our hospital between January 2018 and January 2023.ResultsThe ResultsThe mean aneurysm dome size was 5.29 mm (2–22 mm), and the mean aneurysm neck size was 3.2 12; ATLAS, 14). Postoperative thrombotic complications were observed in 1 patient.
IntroductionFlow diverters (FD) are stent‐type devices that enable the exclusion of intracranial aneurysms in clinical scenarios where coil‐type devices exhibit high failure rates. Adults older than 18 with non‐ruptured intracranial aneurysms were included. years (±13.3). years (±13.3). Neck measurements were in the range of 1.9
IntroductionThe use of detachable coils for endovascular embolization of cerebral aneurysms has become a safe and effective alternative to direct surgical clipping in patients with ruptured aneurysmal subarachnoid hemorrhage. Immediate complete occlusion and occlusion with residual neck was achieved in 66.7%
IntroductionFlow diversion (FD) is commonly used for the treatment of aneurysms involving the ophthalmic segment of the carotid artery (COA). The origin of the ophthalmic artery (OA) in relation to the aneurysm sac can affect recurrence and complications. directly from the aneurysm fundus, B. aneurysm neck, C.
IntroductionInfectious intracranial aneurysms (IIAs), commonly referred to as mycotic aneurysms, are a common sequela of infective endocarditis (IE). were treated with an endovascular approach; 50% underwent onyx embolization, 28.6% underwent n‐BCA embolization, 14.2% Among those IIAs treated, 92.8% 9); (P=0.002).
Statistical analysis was performed to identify predictors of inadequate occlusion.ResultsA total of 51 patients underwent endovascular embolization using the WEB device with a mean follow‐up of 14.9 Ruptured aneurysmal subarachnoid hemorrhage accounted for 15.7% (8/51) of all patients. Retreatment was required in 1 aneurysm.
IntroductionMycotic aneurysms of paraspinal arteries are a rare finding. Furthermore, knowledge regarding the management of paraspinal mycotic aneurysms and the efficacy of endovascular repair of these lesions is scarce.⁴MethodsWe Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023.
IntroductionThe Pipeline Embolization Device (PED) is commonly used for intracranial aneurysm treatment. While its effectiveness for certain types of aneurysms is well‐established, its efficacy for saccular aneurysms remains debatable. The mean aneurysm size was 7.72 The mean age was 55.7 years, and 78.3%
BACKGROUNDCurrently, endovascular treatment of intracranial aneurysms is limited by low complete occlusion rates. The advent of novel endovascular technology has expanded the applicability of endovascular therapies; however, the superiority of novel embolic devices over the traditional Guglielmi detachable coils is still debated.
IntroductionIndications for flow diversion for the treatment of cerebral aneurysms have increased remarkably in recent years.1 1 This has been particularly useful for aneurysms that are difficult to treat via endosaccular or open approaches, such as pseudoaneurysms.2
IntroductionBasilar‐tip aneurysm (BTA) is the most common aneurysm found in the posterior circulation, representing 5–8% of total intracranial aneurysms. Coil embolization (CE) is safer and more efficacious in the treatment of BTAs compared to open surgery but has increased rate of recanalization. vs. 10.7%).
IntroductionInfectious Intracranial Aneurysms (IIAs), commonly referred to as mycotic aneurysms, are a common sequela of infective endocarditis (IE). However, if one is able to embolize and secure IIAs, then that delay between endovascular therapy (EVT) and surgery may be shortened.
Eventually, the PSA of the Internal maxillary artery (IMAX) was embolized, resulting in resolution of the patient's symptoms.MethodsCase ReportResultsA 75‐year‐old male with a history of atrial fibrillation on Eliquis presented to the emergency department after sustaining a gunshot wound to the left face.
IntroductionRuptured aneurysmal SAH accounts up to 80% of nontraumatic SAH, with more than 80% located in the anterior circulation and a mortality rate upwards of 50%.1‐3 1,2,4–6 Despite this, EVT of intracranial aneurysms has its own risk of complications including intraoperative rupture and thromboembolic events.7
IntroductionDual antiplatelet therapy (DAPT) is necessary to minimize the risk of periprocedural thromboembolic complications associated with aneurysmembolization using Pipeline embolization device (PED). of PFT group patients were clopidogrel non‐responders requiring changes in their pre‐embolization DAPT regimen.
A right posterior communication artery aneurysm was discovered incidentally on workup images. The aneurysm was treated using a Woven Endobridge SingleLayer Sphere (SLS) intrasaccular flow disrupter device. On discussing potential options, including observation, the patient opted for endovascular intervention.
AngioCT: a dilated orbito frontal vein, and a venous aneurysm at the anterior third of the superior sagittal sinus. We catheterized ophthalmic artery, and did embolization through it, with a successful result, and with no ophthalmic symptoms after embolization.ConclusionDural arteriovenous fistulas are shunts found from dural vessels.
This may be permanent and may be associated with echocardiographic dyskinesis (aneurysm). LV aneurysm is common in completed, full thickness (transmural) MI, which is what we have here. LV aneurysm puts them at risk for a mural thrombus, which puts them at risk for embolism, especially embolic stroke.
IntroductionSubarachnoid Hemorrhage (SAH) resulting from the spontaneous rupture of an aneurysm is a rare and highly debilitating condition. Despite its severity, patients with aneurysmal SAH remain understudied, particularly concerning the evaluation of the incidence and consequences of subsequent acute kidney injury (AKI).
A Chest CT angiography and a CT angiography of the intra and extracranial vasculature demonstrated an extensive right holohemispheric cerebral AVM, an unruptured 8‐mm basilar artery aneurysm, and multiple enlarged pulmonary arteries with narrow inlet and outlets concerning for pulmonary AVMs.
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. CT chest showed left sided pulmonary embolism and a pulmonary infarct that had previously been mistaken for pneumonia. Instead, he was diagnosed with pneumonia — that turned out to be a left-sided pulmonary embolism that was initially missed.
8290 aneurysmsembolizations were performed (13.5% Mortality percentages were: SAH=20.2%, ICH=25.3%, Ischemic Stroke=15.3%. Rates of Thrombolysis were alarming, but with an increasing tendency: 22969 were performed, from 1.6% in 2017 to 2.3% in 2022 of all ischemic strokes. of all SAH cases).
CT angiogram chest: no aortic dissection or pulmonary embolism. Repeat CT angio chest (not CT coronary, unclear what protocol) showed possible LAD aneurysm and thrombus. No further troponins were measured. Serial chest xrays: progressive bilateral pulmonary edema. No further cath details available.
The patient's heart had significant recovery: Echo : Estimated LVEF 32%, apical wall motion abnormality with diastolic distortion (LV aneurysm), suggestive of old MI. pulmonary embolism, sepsis, etc.), Coronary thrombosis or embolism can result in MINOCA, either with or without a hypercoagulable state. myocarditis).
Mid cavity obstruction in HCM is associated with apical aneurysm, systemic embolism, and arrhythmias. LVOTO is due to septal hypertrophy, SAM, and anterior displacement of mitral valve apparatus. Doppler echo showing LVOT gradient in HCM.
Both of these are very suggestive of " No-Reflow ," or poor microvascular reperfusion due to downstream embolization of microscopic platelet-fibrin aggregates. Perhaps she will not develop an LV aneurysm. However, much ST elevation remains, and there is no re-constitution of R-waves. That remains to be seen.
Object:The introduction of antiplatelet agents is essential in stent-assisted coil embolization (SACE) for the treatment of intracranial aneurysms, and preoperative drug efficacy assessment is important in reducing the risk of ischemic complications. Stroke, Volume 56, Issue Suppl_1 , Page ADP37-ADP37, February 1, 2025.
Look for Vascular Etiology -- think of these while doing H and P: --Bleeding: ruptured AAA, GI bleed, ruptured ectopic pregnancy, other spontaneous bleed such as mesenteric aneurysms. Serious outcomes included death, arrhythmia, myocardial infarction, structural heart disease, pulmonary embolism, and hemorrhage. of ED visits.
His initial high sensitivity troponin I returned at 1300 ng/L and given that his cardiac workup was otherwise unremarkable, a CT was obtained to evaluate for pulmonary embolism and aortic aneurysm or dissection but this too was unrevealing. Another EKG was also obtained. ECG at time 82 minutes: What do you think?
No thoracic aortic hematoma, aneurysm or dissection. No pulmonary embolism is identified. While in the ED, patient's pain worsened to previous severity of 6/10 pain and improved to 3/10 on NTG drip. CT Angio Chest IMPRESSION 1. There are moderate coronary artery calcifications.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content