This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The aim was to characterize the electrovectorcardiographic pattern of ventricular aneurysms in ischemic cardiopathy by analyzing the cardiac ventricular repolarization. The electrovectorcardiographic parameters showed high accuracy for recognizing left ventricular aneurysms in ischemic heart disease.
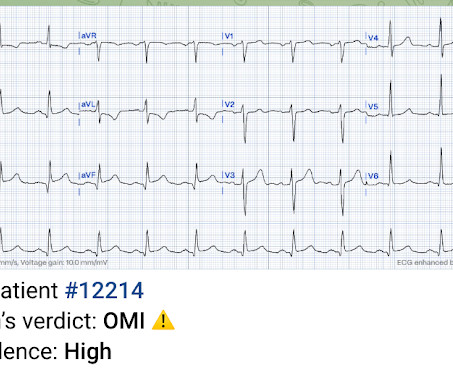
The only alternative is old inferior MI with persistent ST-Elevation, or inferior aneurysm morphology. Inferior Aneurysm morphology is incredibly hard to differentiate from Acute OMI, but you should suspect it whenever there are well-formed inferior Q-waves. Unlike anterior aneurysm, a QS-wave is uncommon. Learning Points: 1.
Aim:This study investigates the prevalence of isolated interventricular membranous septal (IVMS) aneurysms detected via echocardiography and assesses the associated stroke risk without other classical risk factors.Methods:We searched the echocardiography database at Mount Sinai Morningside from January 2017 to September 2023.
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
Introduction:Sinus of Valsalva aneurysm (SVA) accounts for 3.5% Her ejection fraction was 66% ejection fraction with a fistula between the right sinus of Valsalva and the right atrium on transthoracic echocardiogram (TTE) which was also seen on transesophageal echocardiogram (TEE). of all congenital cardiac anomalies.
Inferior LV "aneurysm" morphology Electrocardiographic "LV Aneurysm" morphology simply means "persistent ST elevation after previous MI." Not all such ECGs represent anatomic aneurysms (on echo this is "diastolic dyskinesis"), but do generally represent an area of dense akinesis on echocardiogram.
One very useful adjunct is ultrasound: Echo of his heart can distinguish aneurysm from acute MI by presence of diastolic dyskinesis, but it cannot distinguish demand ischemia from ACS. Furthermore, notice the well-formed Q-waves in inferior leads. These must raise suspicion of old MI with persistent ST elevation.
The old ECG has a Q-wave with persistent ST elevation in lead III, and some reciprocal ST depression (typical for aneurysm morphology). This is "Persistent ST elevation after previous MI" or "LV aneurysm morphology". LV aneurysm is very different for inferior vs. anterior MI. Transient ST elevation is very hazardous.
The EKG is diagnostic of acute inferior, posterior, and lateral OMI superimposed on “LV aneurysm” morphology. Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. A formal echocardiogram for patient 2 showed normal LV size, wall thickness, and global systolic function.
An echocardiogram showed severely reduced global systolic function with an EF of 20-25% and an LV apical thrombus. The LV aneurysm morphology persists. An echocardiogram showed an EF of 20-25%. Troponin I values trended from 0.262 to 0.746 ng/mL in 6 hours (URL for this assay is 0.034 ng/mL). This is the RAO caudal projection.
But the well-formed Q-wave and the presence of a normal T-wave in inferior leads led me to believe this was Old Inferior MI with persistent ST Elevation, otherwise known as inferior LV aneurysm. Anterior LV aneurysm is much easier to recognize because the Q-wave is usually a QS-wave (no R-wave at all), in at least one lead.
Kawasaki Disease Case : Angela Khidhir, DO, MSc (USA) presented a compelling case on ACS and tamponade potentially linked to Kawasaki disease-related Coronary Artery Aneurysm. This debate underscored the growing role of CSP despite the current limited evidence supporting it. Memorial Lecture for Dr. Alain Cribier: Prof.
No further echocardiograms were available after cath. The full thickness infarction with LV aneurysm morphology places him at a higher risk for short and long term complications (e.g., Free wall rupture, VSD, Dresslers Syndrome, chronic CHF, anatomic LV aneurysm, LV thrombus, stroke, etc). Teaching points: 1.
An echocardiogram showed no hemopericardium, but D oppler showed a new small ventricular septal defect with left to right shunting. Additionally , these patients have a high incidence of LV aneurysm with mural thrombus. No resolution of ST elevation. The T-waves are persistently positive. Bedside echo may detect these in a timely way.
QS waves from V2-V5 consistent with LV aneurysm morphology. Echocardiogram: EF 50%, akinesis of mid-apical anteroseptal, inferior, and inferoseptal myocardium. There is a QS-waves in V2: is this "Old MI with persistent STE (otherwise known as LV aneurysm morphology)"? Normal RV, no valve stenosis or regurgitation. 6.5 = 0.38.
No prior echocardiogram was available for comparison. Is LVH like left ventricular aneurysm? However, an analogous rule for identifying superimposed ACO of the LAD in the presence of persistent STE after prior MI (aka “ left ventricular aneurysm ,” or LVA) was just validated. ECG #3 at 0018 hours. Am J Emerg Med. 2007;25(7):859.e1-e859.e7.
Echocardiogram showing thickened interventricular septum and mitral regurgitation in HCM. Mid cavity obstruction in HCM is associated with apical aneurysm, systemic embolism, and arrhythmias. SAM in HCM Systolic anterior movement of mitral valve occurs in 30 – 60%, but it is not specific. Doppler echo showing LVOT gradient in HCM.
Echocardiogram in parasternal long axis view shows dilated left ventricle, left atrium, aorta and a small portion of the right ventricle, which is usually the outflow region. Eccentric aortic regurgitation has been reported in ascending aortic aneurysm. PISA method has been described in another video on this channel.
Next day echocardiogram showed inferolateral hypokinesia with an EF of %45-50. On echocardiogram you will not see a "posterior" hypokinesia (will see "inferolateral") and, as in this case, LCx may not give the blood supply of basal inferior segment (formerly called "posterior"). The patient recovered well.
You might think it is "Old MI with persistent ST Elevation" (otherwise known as "LV aneurysm" morphology.") That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. Formula value = 20.89, which is much higher than the cutpoint of 18.2
Look for Vascular Etiology -- think of these while doing H and P: --Bleeding: ruptured AAA, GI bleed, ruptured ectopic pregnancy, other spontaneous bleed such as mesenteric aneurysms. Results : Electrocardiograms (99%), telemetry (95%), cardiac enzymes (95%), and head computed tomography (CT) (63%) were the most frequently obtained tests.
There is limited literature regarding cases of giant coronary artery aneurysms (GCAAs), and instances of giant coronary artery pseudoaneurysms caused by trauma are exceedingly rare. Here is a case presentation of an adult male who developed a giant coronary artery pseudoaneurysm following trauma.
An echocardiogram revealed the heart condition that would define much of his early life: severe congenital heart defects. After countless tests, doctors confirmed that it wasnt a seizure, but an aneurysm in his LVOT (left ventricular outflow tract). That test revealed an irregular heart rate, prompting a more in-depth evaluation.
There are no Q-waves to suggest old inferior MI, or inferior aneurysm as the etiology of the ST Elevation. Smith : I would say this STE with T-wave inversion (suggesting reperfusion) is "between" active and reperfused inferior OMI, and with persistent symptoms or instability, it is active and acute until proven otherwise.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content