This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
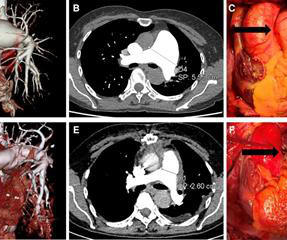
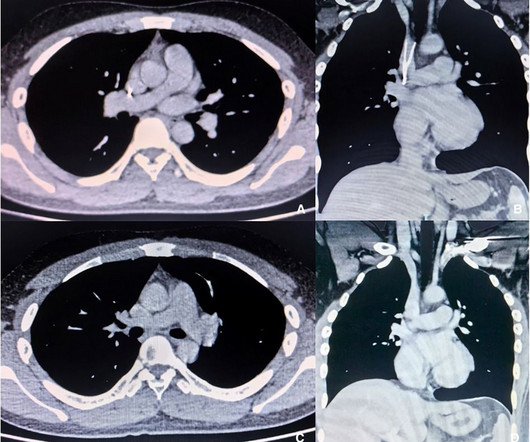
Idiopathic pulmonaryaneurysm is a clinically rare condition characterized by an unknown etiology and episodic occurrence. Despite its rarity, idiopathic pulmonary artery aneurysm poses potential risks to patients. Subsequently, she underwent surgical treatment.
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. Smith : Old inferior MI with persistent ST Elevation ("inferior aneurysm") has well-formed Q-waves. What do you think?
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Ten days later the patient returned with worsening pleuritic chest.
Ken (below) is appropriately worried about pulmonary embolism from the ECG. What I had not told him before he made that judgement is that the patient also had ultrasound B-lines of pulmonary edema. LV aneurysm has QS-waves, so this couldn't be LV aneurysm, right? Finally, the presentation is dyspnea, not chestpain.
He had no chestpain. He was in acute distress from pulmonary edema, with a BP of 180/110, pulse 110. He had diffuse crackles on exam and B-lines on chest ultrasound, and chest x-ray also confirmed pulmonary edema. The hypertension alone is the likely etiology of the pulmonary edema.
Preoperative ultrasonography and CT examination revealed that the filter retraction hook was very likely to penetrate the SVC wall and its tip was very close to the right pulmonary artery. During this procedure, the patient experienced discomfort, such as chestpain and palpitations, but these symptoms disappeared when procedure completed.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." At some point he returned with chestpain, and all these findings were put into place. Many MI do not have chestpain 4. He was discharged and returned again.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. Additionally , these patients have a high incidence of LV aneurysm with mural thrombus. There was some SOB. He had walked into the ED (did not use EMS).
Look for Vascular Etiology -- think of these while doing H and P: --Bleeding: ruptured AAA, GI bleed, ruptured ectopic pregnancy, other spontaneous bleed such as mesenteric aneurysms. Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. CONCLUSIONS: Many tests for syncope have a low diagnostic yield.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. When there are QS-waves, one should always think about LV aneurysm, but ST to QRS ratio and T-wave to QRS ratio are far too large and not compatible with left ventricular aneurysm. He presented to the emergency department for evaluation.
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chestpain that started while working at his desk. He reported the crushing chestpain radiated down his left arm. He presented to the ED for evaluation chestpain. Pain was improved but not gone upon arrival.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content