This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
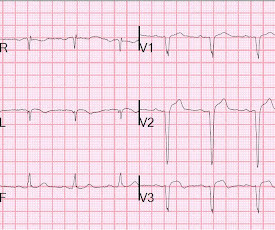
No ChestPain, but somnolent. There are QS-waves in V1-V3 suggesting old anterior MI with persistent ST Elevation (LV aneurysm morphology), but I have written a couple papers showing that in LV aneurysm, the T-wave is not > 0.36 But the T-waves in LV aneurysm are not this big. Smith : "What was the outcome?"
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. Smith : Old inferior MI with persistent ST Elevation ("inferior aneurysm") has well-formed Q-waves. What do you think?
A 29 year old male presented with 6 hours of stuttering chestpain, constant for the last hour, worse with breathing. Take home point here : Obtain an ECG on anyone with chestpain. 3) Q-waves are independently associated with worse outcomes (78% relative increase in 90-day mortality in Armstrong et al.)
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6 mg/dL, K 3.5
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. TIMI flow alone cannot be used as an outcome definition for OMI or STEMI. =
This case was recently posted by Tyron Maartens on Facebook EKG club (he agreed to let me post it here), with the following clinical information: "42 year old male with two weeks of intermittent chest discomfort, awoke 4 hours prior to this ECG with a more severe, heavy chestpain (5/10). BP 112/80, SpO2 100%. It is not chronic.
A 20-something male presented from an outside facility with Chestpain. He came with this ECG from the outside facility, recorded 1 hour after pain onset: There is at least 2 mm of inferior ST elevation, with reciprocal ST depression in aVL, ST flattening in V4-V6, and T-wave inversion in V2. A coronary aneurysm was found.
He had no chestpain. The computer read is: **Acute MI ** The protocol for prehospital activation in the EMS system that this patient presented to requires 2 elements: 1) Chestpain 2) A computer read of **Acute MI ** Only 1 of 2 was present, so there was no prehospital activation. The patient was transported to the ED.
No patient with chestpain should be sent home without troponin testing. The LV aneurysm morphology persists. The patient was sent home with a prescription for omeprazole to treat presumed peptic disease. He spent the following weeks with continued episodic heartburn and worsening dyspnea on exertion.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
This is one case where it made a difference: Right Ventricular MI seen on ECG helps Angiographer to find Culprit Lesion Nevertheless, it is sometimes a fun academic exercise to try to predict the infarct artery: An elderly patient had onset of chestpain one hour prior. See more such cases of RBBB with LV aneurysm here.
Persistent ST elevation 3 days after a nearly transmural MI portends possible LV aneurysm. This 42 yo diabetic male presented with cough and foot pain. Symptoms have been prolonged but intermittent, and there has been little chestpain, if any. He had been awakened by cough at 3 AM 2 days earlier.
Full case details and outcomes are below. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Repeat 0157 with ongoing chestpain: Basically the same features diagnostic of LAD occlusion. Physician: "No STEMI."
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
When we observed that bicuspid aortic valve is kind of a risk marker for this group with bad outcomes, we specifically wanted to see whether young individuals who present clinically due to problems related to bicuspid aortic valve disease may also have rare genetic variants that predict complications such as needing valve surgery.”
An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL." Case 3 : Male in 30's with chestpain, cough, and fever. What do you think? EMS recorded the following ECG: What do you see?
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. such Q-waves are associated with larger MI and worse outcomes (2. Additionally , these patients have a high incidence of LV aneurysm with mural thrombus.
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chestpain for 1.5 Perhaps she will not develop an LV aneurysm. A cutoff of 9 mm for inferior AMI and 13 mm for anterior AMI predicted worse outcome. Findings: Greater reciprocal ST depression correlated strongly with poor outcome.
On the other hand, a positive troponin like that with ongoing chestpain, even in the absence of any ECG findings of Acute MI or OMI, is an indication for the cath lab. What is needed is to feed the AI algorithms huge numbers of tracings with verfiable outcomes. Angiography confirmed LAD OMI and thrombus.
You might think it is "Old MI with persistent ST Elevation" (otherwise known as "LV aneurysm" morphology.") That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. What's the story?"
Look for Vascular Etiology -- think of these while doing H and P: --Bleeding: ruptured AAA, GI bleed, ruptured ectopic pregnancy, other spontaneous bleed such as mesenteric aneurysms. Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Abnormal ECG – looks for cardiac syncope.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. When there are QS-waves, one should always think about LV aneurysm, but ST to QRS ratio and T-wave to QRS ratio are far too large and not compatible with left ventricular aneurysm. He presented to the emergency department for evaluation.
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chestpain that started while working at his desk. He reported the crushing chestpain radiated down his left arm. He presented to the ED for evaluation chestpain. Pain was improved but not gone upon arrival.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content