This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
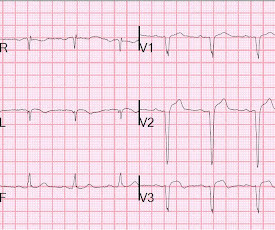
No ChestPain, but somnolent. There are QS-waves in V1-V3 suggesting old anterior MI with persistent ST Elevation (LV aneurysm morphology), but I have written a couple papers showing that in LV aneurysm, the T-wave is not > 0.36 But the T-waves in LV aneurysm are not this big. LV Aneurysm vs New Infarction?
A 60-something male presented stating that he had had chestpain that morning which awoke him from sleep but then resolved after several minutes. He has had similar pain in the past which he attributed to acid reflux. He is pain free now. The patient is pain free at the time of this ECG: What do you think?
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. Smith : Old inferior MI with persistent ST Elevation ("inferior aneurysm") has well-formed Q-waves. What do you think?
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Do either, both, or neither have occlusion MI? Vitals were normal.
Clinical introduction A man in his 40s with a history of hyperlipidaemia presented with intermittent, dull left-sided chestpain for 2 weeks that was not consistently exertional. Physical examination, an ECG, basic laboratories and a chest X-ray were unremarkable. He did not smoke or use alcohol or illicit drugs.
Increased Risk of Aneurysms : Chronic high blood pressure can weaken the walls of your arteries, leading to bulging areas known as aneurysms. If an aneurysm ruptures, it can cause life-threatening internal bleeding. This condition reduces blood flow to the heart, increasing the risk of angina (chestpain) and heart attacks.
52-year-old lady presents to the Emergency Department with 2 hours of chestpain, palpitations & SOB. However, old MI w/aneurysm morphology (persistent ST-Elevation) can look just like this. Old MI w/Aneurysm will show moderate ST Elevation, as seen here. Notice also that no lead has 1 mm of ST elevation.
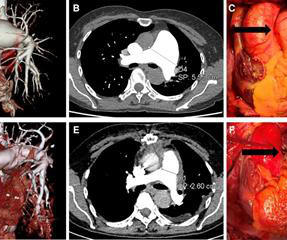
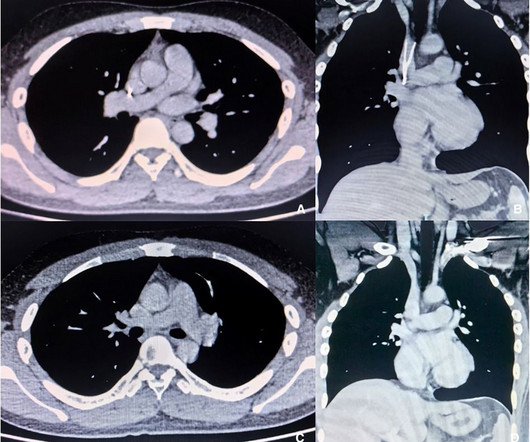
Idiopathic pulmonary aneurysm is a clinically rare condition characterized by an unknown etiology and episodic occurrence. Despite its rarity, idiopathic pulmonary artery aneurysm poses potential risks to patients. Subsequently, she underwent surgical treatment.
A 29 year old male presented with 6 hours of stuttering chestpain, constant for the last hour, worse with breathing. Take home point here : Obtain an ECG on anyone with chestpain. He had no medical history. What is the diagnosis? Sometimes you will find an obvious STEMI. He has persistent ST elevation.
LV aneurysm has QS-waves, so this couldn't be LV aneurysm, right? RBBB makes it mandatory that there are R'-waves even in the presence of LV aneurysm. Additionally, it is very difficult to differentiate subacute reperfused OMI from LV aneurysm: both have Q-waves and inverted T-waves. This is HIGHLY suspicious for OMI.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6 mg/dL, K 3.5
Sinus of Valsalva aneurysm (SVA) is an extremely rare condition, and its rupture causes acute symptoms such as chestpain and dyspnea. Ruptured SVA is frequently associated with other congenital defects.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. Isn't it amazing?? hours earlier? Don’t Ignore Bedside Echo Results! —
The medics stated he had been nauseated and diaphoretic, but he did not have any chestpain or SOB. The only alternative is old inferior MI with persistent ST-Elevation, or inferior aneurysm morphology. Unlike anterior aneurysm, a QS-wave is uncommon. Unlike anterior aneurysm, a QS-wave is uncommon.
An elderly woman presented with chestpain that radiated to the back for several hours. The first troponin returned at 0.099 ng/mL (elevated, consistent with Non-Occlusion MI) Providers were concerned with aortic dissection, so they order a chest aorta CT. Here is here initial ECG: There is only a nonspecific flat T-wave in aVL.
Written by Pendell Meyers, with edits by Steve Smith A man in his early 40s with history of MI s/p PCI presented with bilateral anterior chestpain described as burning and belching with no radiation since last night starting around 11pm (roughly 11 hours ago). The patient was still with ongoing chestpain at the time ECG #1 was done.
This case was recently posted by Tyron Maartens on Facebook EKG club (he agreed to let me post it here), with the following clinical information: "42 year old male with two weeks of intermittent chest discomfort, awoke 4 hours prior to this ECG with a more severe, heavy chestpain (5/10). BP 112/80, SpO2 100%. It is not chronic.
70 yo with h/o MI, recent CABG, has acute onset of chestpain. The differential is wider, however, and mostly includes "old MI with persistent ST elevation," otherwise known as "left ventricular aneurysm morphology". in acute MI, and almost always lower in LV aneurysm. What is the most likely diagnosis?
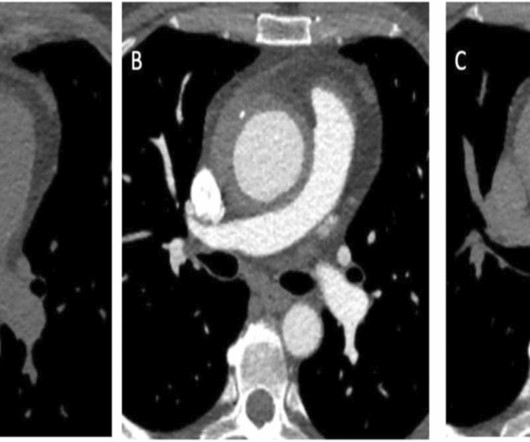
A 54-year-old female presented with recurrent abdominal pain and new onset chestpain. Chest computed-tomography angiogram detected a thoracic aortic aneurysm with suspected Type A intramural hematoma (IMH) versu.
A 20-something male presented from an outside facility with Chestpain. He came with this ECG from the outside facility, recorded 1 hour after pain onset: There is at least 2 mm of inferior ST elevation, with reciprocal ST depression in aVL, ST flattening in V4-V6, and T-wave inversion in V2. A coronary aneurysm was found.
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
He had no chestpain. The computer read is: **Acute MI ** The protocol for prehospital activation in the EMS system that this patient presented to requires 2 elements: 1) Chestpain 2) A computer read of **Acute MI ** Only 1 of 2 was present, so there was no prehospital activation. The patient was transported to the ED.
The patient reported no chestpain or shortness of breath. Cystic formation of the foramen ovale Aortic sinus aneurysm Left. Clinical introduction A woman is her 60s with no medical history presented to the hospital with palpitations and occasional nausea. Observations revealed a normal temperature of 36.5°C
During this procedure, the patient experienced discomfort, such as chestpain and palpitations, but these symptoms disappeared when procedure completed.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
This 54 year old patient with a history of kidney transplant with poor transplant function had been vomiting all day when at 10 PM he developed severe substernal crushing chestpain. He presented to the Emergency Department with a blood pressure of 111/66 and a pulse of 117. He had this ECG recorded.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Patient 2 , EKG 1: What do you think?
Although diagnostic of MI, it is highly suspicious for " Old inferior MI with persistent ST Elevation" or "inferior aneurysm morphology" because of the well-formed Q-waves and the flat T-waves. To repeat: in contrast, anterior aneurysm is much more easily distinguished from acute MI due to the QS-waves. There are well-formed Q-waves 3.
This is one case where it made a difference: Right Ventricular MI seen on ECG helps Angiographer to find Culprit Lesion Nevertheless, it is sometimes a fun academic exercise to try to predict the infarct artery: An elderly patient had onset of chestpain one hour prior. See more such cases of RBBB with LV aneurysm here.
But the well-formed Q-wave and the presence of a normal T-wave in inferior leads led me to believe this was Old Inferior MI with persistent ST Elevation, otherwise known as inferior LV aneurysm. Anterior LV aneurysm is much easier to recognize because the Q-wave is usually a QS-wave (no R-wave at all), in at least one lead.
Persistent ST elevation 3 days after a nearly transmural MI portends possible LV aneurysm. This 42 yo diabetic male presented with cough and foot pain. Symptoms have been prolonged but intermittent, and there has been little chestpain, if any. He had been awakened by cough at 3 AM 2 days earlier.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." At some point he returned with chestpain, and all these findings were put into place. Many MI do not have chestpain 4. He was discharged and returned again.
3 hours prior to calling 911 he developed typical chestpain. The old ECG has a Q-wave with persistent ST elevation in lead III, and some reciprocal ST depression (typical for aneurysm morphology). This is "Persistent ST elevation after previous MI" or "LV aneurysm morphology".
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chestpain that started while mowing the lawn. TOP Initial ECG of this 60-year old man with a history of prior MI, who presented with new-onset chestpain.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Here is the clinical informaton on ECG 2: A man in his 50s presented to the Emergency Department with acute chestpain that started within the past few hours.
Case 1 A middle aged woman presented with acute chestpain and shortness of breath, unclear time since onset, and likely with episodic symptoms off and on throughout the day. QS waves from V2-V5 consistent with LV aneurysm morphology. Submitted by anonymous, written by Pendell Meyers. Additional case by Smith.
Subsequently, he developed chestpain with hypotension, diffuse ST elevations on ECG, and hsTropI of 638 ng/L. Cervical adenopathy and hepatitis are more common in adults while coronary artery aneurysms are rarer. Labs include WBC count 13320/cmm with 85% neutrophils, total bilirubin 13.1 mg/dL, direct bilirubin 9.3
He denied fevers and chills, abdominal pain, chestpain, or SOB. This may be permanent and may be associated with echocardiographic dyskinesis (aneurysm). LV aneurysm is common in completed, full thickness (transmural) MI, which is what we have here. Patient stated his dry weight is around 85 kg.
This can lead to complications such as blocked, reduced, or backward blood flow through the heart chambers, causing shortness of breath, chestpain, fainting, and difficulty exercising. In more severe cases, the disease can lead to an aortic dissection, or tear in the aorta, a life-threatening condition.
No patient with chestpain should be sent home without troponin testing. The LV aneurysm morphology persists. The patient was sent home with a prescription for omeprazole to treat presumed peptic disease. He spent the following weeks with continued episodic heartburn and worsening dyspnea on exertion.
What do you think of this ECG in a patient with chestpain? Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chestpain. The pain had been mild and intermittent for 2 weeks, but had become more intense on the night of presentation. Is the ST elevation due to LVH?
An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL." Case 3 : Male in 30's with chestpain, cough, and fever. What do you think? EMS recorded the following ECG: What do you see?
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. Additionally , these patients have a high incidence of LV aneurysm with mural thrombus. There was some SOB. He had walked into the ED (did not use EMS).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content