This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
High bloodpressure, also known as hypertension, is a common condition that affects millions of people worldwide. Understanding how high bloodpressure impacts your heart and learning to manage it can significantly reduce your risk of heart disease and improve your overall health. What Is High BloodPressure?
No ChestPain, but somnolent. There are QS-waves in V1-V3 suggesting old anterior MI with persistent ST Elevation (LV aneurysm morphology), but I have written a couple papers showing that in LV aneurysm, the T-wave is not > 0.36 But the T-waves in LV aneurysm are not this big. LV Aneurysm vs New Infarction?
The patient reported no chestpain or shortness of breath. °C and a normal bloodpressure of 123/83 mm Hg. Cystic formation of the foramen ovale Aortic sinus aneurysm Left. Clinical introduction A woman is her 60s with no medical history presented to the hospital with palpitations and occasional nausea.
He had no chestpain. The computer read is: **Acute MI ** The protocol for prehospital activation in the EMS system that this patient presented to requires 2 elements: 1) Chestpain 2) A computer read of **Acute MI ** Only 1 of 2 was present, so there was no prehospital activation. The patient was transported to the ED.
This 54 year old patient with a history of kidney transplant with poor transplant function had been vomiting all day when at 10 PM he developed severe substernal crushing chestpain. He presented to the Emergency Department with a bloodpressure of 111/66 and a pulse of 117. He had this ECG recorded.
These are all findings that can be expected with left ventricular aneurysm. Therefore — Just because a patient remains awake and alert with an adequate bloodpressure for an extended period of time does not rule out the possibility sustained VT. There are QS-waves in V1-V4 with a fragmentation/notch in the last part of the QRS.
Still Irregular Bloodpressure during these rhythms was adequate; there was no shock. Old MI with persistent ST Elevation (LV aneurysm morphology) can look like acute MI 2. Not all anterior LV aneurysm has a QS-wave. LV Aneurysm? 9 Hours of ChestPain and Deep Q-waves: Is it too late for Thrombolytics?
Look for Vascular Etiology -- think of these while doing H and P: --Bleeding: ruptured AAA, GI bleed, ruptured ectopic pregnancy, other spontaneous bleed such as mesenteric aneurysms. Vasovagal predisposition (warm crowded place, prolonged standing, fear, emotion, pain: (-1) 2. h/o heart disease (+1) 3.
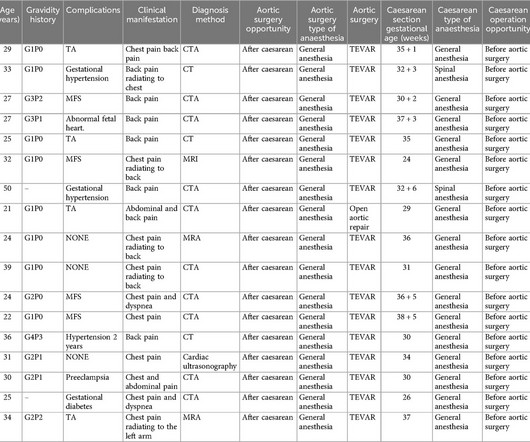
It leads to thickening and loss of elasticity of the arterial wall, and eventually vascular occlusion, aneurysm or dissection formation. Her bloodpressure was 209/73mmHg and could not be lowered with Urapidil, therefore she was diagnosed with complex Stanford type B aortic dissection. She had TA for five years.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content