This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BACKGROUND:Aberrant BMPR2 (bone morphogenetic protein receptor 2) signaling is associated with the pathogenesis of pulmonary hypertension. By contrast, mice with smooth muscle cell-specificSmad4deletion had no pulmonary hypertension but rather displayed evident aorticaneurysm and dissection.
Patients with pulmonary atresia and ventricular septal defect (PA/VSD) are prone to progressive aortic dilation. However, there are relatively few reports of progressive development of aorticaneurysm or aorti.
Pulmonary agenesis D. Ascending aorticaneurysm Answer: As the patient is a known case of arterial tortuosity syndrome, which is a rare hereditary disorder characterised by lengthening, dilatation and tortuosity of large and medium-sized arteries. The other images of the aneurysm are shown in. Left lung collapse C.
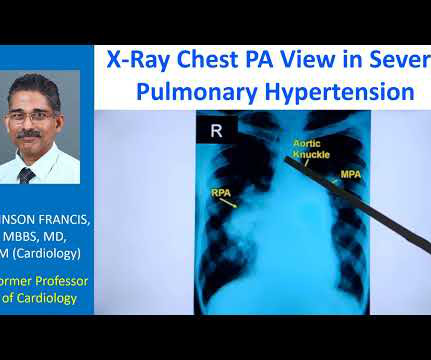
The striking finding is the huge enlargement of the right pulmonary artery, almost aneurysmal dilatation of right pulmonary artery. Main pulmonary artery is also grossly dilated. And you can see left pulmonary artery shadow and rest of it is not seen here. This is the aortic knuckle.
Cardiovascular neurocristopathy, i.e., cardiopathy and vasculopathy, associated with the NCC could occur in the form of (1) cardiac septation disorders, mainly the aortico-pulmonary septum; (2) great vessels and vascular disorders; (3) myocardial dysfunction; and (4) a combination of all three phenotypes.
By these mechanisms, SMC-MR promotes disease progression in models of aging-associated vascular stiffness, vascular calcification, mitral and aortic valve disease, pulmonary hypertension, and heart failure. While rarely tested, when sexes were compared, the mechanisms of SMC-MR-mediated disease were sexually dimorphic.
An intra-aortic balloon pump was placed, and the patient was taken for immediate surgical repair but did not survive. Rupture can be either free wall rupture (causing tamonade) or septal rupture, causing ventricular septal defect with left to right flow and resulting pulmonary edema and shock. 3) Oliva et al. (4)
CT angiogram chest: no aortic dissection or pulmonary embolism. Serial chest xrays: progressive bilateral pulmonary edema. Repeat CT angio chest (not CT coronary, unclear what protocol) showed possible LAD aneurysm and thrombus. No further troponins were measured. No further cath details available.
There are no Q-waves to suggest old inferior MI, or inferior aneurysm as the etiology of the ST Elevation. I suspect pulmonary edema, but we are not given information on presence of B-lines on bedside ultrasound, or CXR findings. Smith : "decompensation" of aortic stenosis might have initiated this entire cascade.
BackgroundType I endoleaks (T1ELs) and type II endoleaks (T2ELs) are among the most severe complications that occur after thoracic endovascular aortic repair (TEVAR) and open surgery. Contrast-enhanced computed tomography angiography of the entire aorta confirmed the diagnosis of aortic disease (e.g.,
Look for Vascular Etiology -- think of these while doing H and P: --Bleeding: ruptured AAA, GI bleed, ruptured ectopic pregnancy, other spontaneous bleed such as mesenteric aneurysms. Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. heart auscultation (aortic stenosis); c. orthostatic vitals b.
His initial high sensitivity troponin I returned at 1300 ng/L and given that his cardiac workup was otherwise unremarkable, a CT was obtained to evaluate for pulmonary embolism and aorticaneurysm or dissection but this too was unrevealing. Also: electrical instability, pulmonary edema, or hypotension.
When there are QS-waves, one should always think about LV aneurysm, but ST to QRS ratio and T-wave to QRS ratio are far too large and not compatible with left ventricular aneurysm. Larger shunt volume means less blood exiting the left ventricle through the aortic valve and lower cardiac output. This ECG shows a lot of "acuity".
No thoracic aortic hematoma, aneurysm or dissection. No pulmonary embolism is identified. While in the ED, patient's pain worsened to previous severity of 6/10 pain and improved to 3/10 on NTG drip. CT Angio Chest IMPRESSION 1. There are moderate coronary artery calcifications.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content