This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
First hs troponin I returned 108 minutes after ED arrival and was normal : (12 ng/L) _ No "upstream" P2Y12 were given in the ED ("upstream" means "before the angiogram "defines" the coronary anatomy). Here are other very interesting posts: Wellens' syndrome: to stent or not?
We aimed to develop a 3D printed ICAD model including realistic features to provide an optimal simulation phantom for research and training purposes.MethodsStereolithography 3D printing technique was used to create a resin neurovascular model based on vascular anatomies extracted from anonymized CTA images.
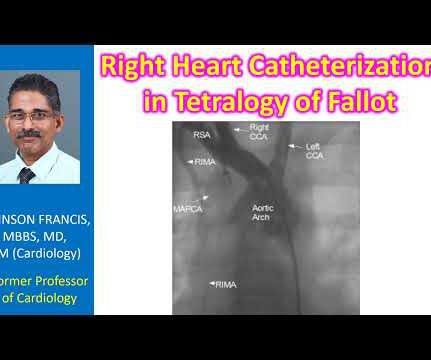
Diagnostic cardiac catheterization may be needed especially in tetralogy of Fallot with pulmonary atresia, to assess the pulmonary anatomy, including size and distribution of peripheral pulmonary arteries. Stenting of the patent ductus arteriosus can be considered in neonatal period for improving oxygen saturation till corrective surgery.
The left circumflex had 80% proximal stenosis with minimal luminal irregularities in the mid to distal portion. After guidewire crossing, balloon angioplasty was performed, and a drug-eluting stent was deployed. An intravascular ultrasound was also performed, which was negative for vessel dissection.
60-something with h/o MI and stents presented with chest pain radiating to the back and nausea/vomiting. The cath lab was activated: Result: Thrombotic 95% stenosis at the ostium of a small LPL2 with 70% stenosis at the LPL2/LPDA bifurcation in the distal/AV groove Cx Tubular 70% stenosis in the mid-circumflex. (In
They found an acute lesion of the LAD at the site of the prior stents, including 70% proximal LAD lesion and 95% mid-LAD stenosis with TIMI 3 flow at the time of cath. The LAD lesion was acute and required 3 stents to restore flow. because if it does, then urgent cath to define the anatomy is clearly indicated.
Here I annotate it: This shows 100% occluded circumflex (red arrow) and a 90% stenosis of the LAD (Yellow arrow). The LAD was thought to be not thrombotic, but a chronic tight stenosis. Initial priorities in this patient were clearly to determine the anatomy — and reestablish coronary perfusion. Sotalol prolongs the QT 7.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content