
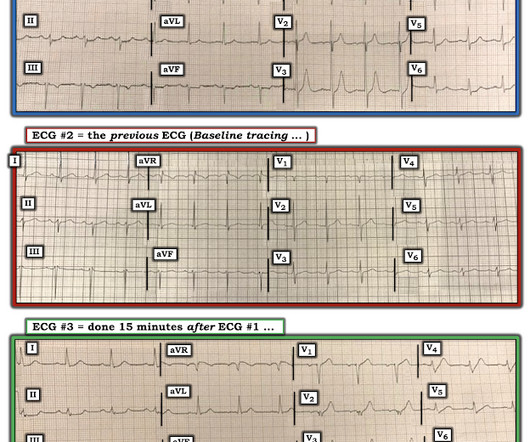
Chest pain and new regional/reciprocal ECG changes compared to previous ECGs: code STEMI?
Dr. Smith's ECG Blog
NOVEMBER 27, 2023
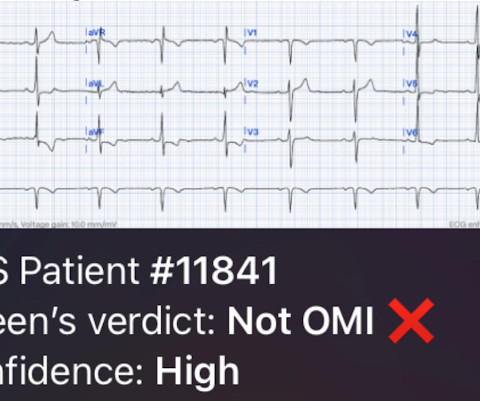
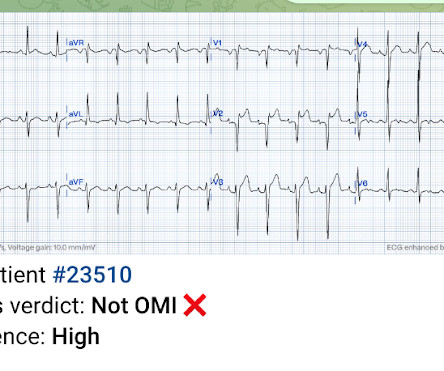
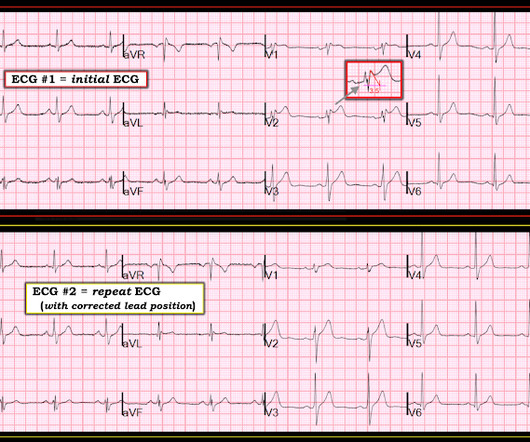
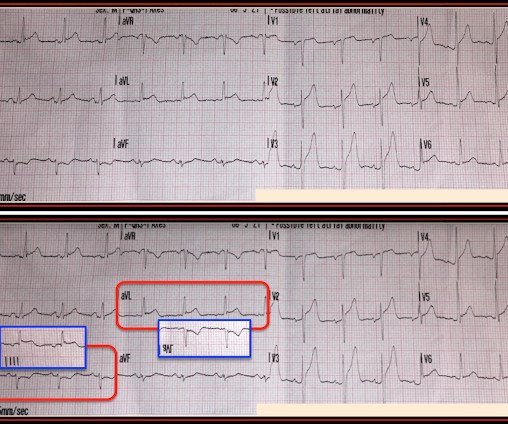
The biggest problem with STEMI criteria are false negatives – because this costs patient’s myocardium, with greater mortality and morbidity. For this reason, ECGs need first to be interpreted in isolation, and then applied to the patient. Could this false positive cath lab activation been prevented? GREAT case by Dr. McLaren!
























Let's personalize your content