This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The biggest problem with STEMI criteria are false negatives – because this costs patient’s myocardium, with greater mortality and morbidity. For this reason, ECGs need first to be interpreted in isolation, and then applied to the patient. Could this false positive cath lab activation been prevented? GREAT case by Dr. McLaren!
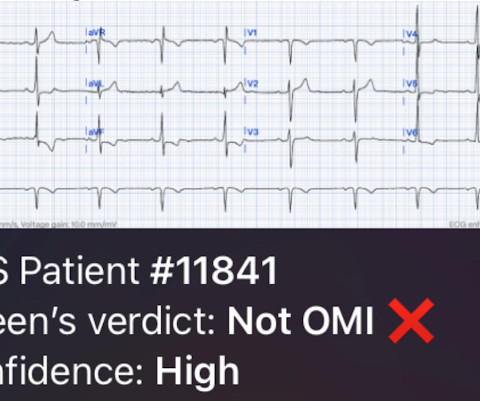
This ECG was texted to me with the implied question "Is this a STEMI?": I responded that it is unlikely to be a STEMI. Septal STEMI often has ST depression in V5, V6, reciprocal to V1. Then combine with clinical presentation and low pretest probability 2 Saddleback STEMIs A Very Subtle LAD Occlusion.T-wave wave in V1??
They wanted to know if I would like them to activate the outside hospital's "STEMI alert." But of course, this is not a STEMI by definition as it does not meet STEMI criteria. The STEMI guidelines do state that hyperacute T-waves "may indicate early acute myocardial infarction" but do not discuss it as a "STEMI equivalent."
Over the next few hours, four other general cardiologists "signed off on the initial ECG without recognizing STEMI." Learning Points: STEMI criteria misses 25-40% of OMI, like this case for example. A millimeter definition of acute STEMI should not be needed to justify the need for prompt cardiac catheterization.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. This one is easy for the Queen.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. Large STEMI are approximately 30-80.
Will evolve into STEMI by prothrombotic trigger of lytic agent ECG will get normalised with clinical stability in some Nothing happens. Majority of Wellens end up as NSTEMI, statistics tells us about 20% of them can be STEMI in incognito mode demanding lysis or emergency PCI. ECG will remain same. How to manage Wellen syndrome?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
Looking at the location of ST elevation ( ie, in the inferior leads — and in V4,5,6 ) — and the location of ST depression ( ie, in leads I,aVL; V1,V2 ) — this ECG picture suggests an ongoing acute infero - postero - lateral STEMI. What is S hark F in M orphology ? Cardiopulmonary resuscitation was promptly started — but was unsuccessful.
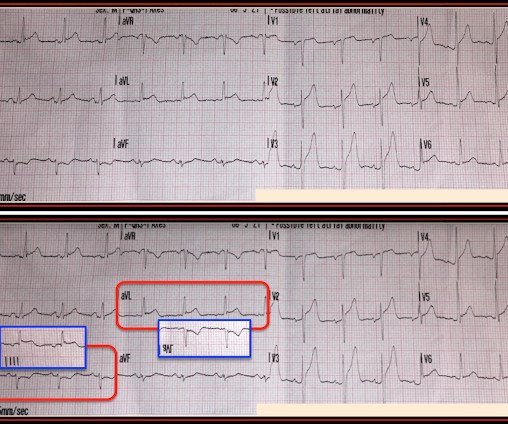
There’s mild inferior ST elevation in III that doesn’t meet STEMI criteria, but it’s associated with ST depression in aVL and V2 that makes it diagnostic of infero-posterior Occlusion MI (from either RCA or circumflex)– accompanied by inferior Q waves of unknown age. Are there any signs of occlusion or reperfusion?
Intra-procedural data included access route, coronary anatomy, lesion complexity, number of stents deployed, door-to-balloon time for primary PCI, and any intra-procedural complications. Pre-procedural data included patients’ baseline characteristics (age, gender, clinical presentation and comorbidities).
This qualifies as " dynamic " ST-T wave change — and in a patient with new chest pain, this is indication for prompt cath to define the anatomy and ensure reperfusion. ECG Blog #294 — How to tell IF the "culprit" artery has reperfused. ECG Blog #194 — AIVR as a sign that the "culprit" artery has reperfused.
Here it is: The computer reads STEMI What do you think? More from the medic: "LifePak 15 interpretation was STEMI. My response: "I think it is very worrisome for STEMI." It meets STEMI criteria even for a male under age 40, with STE 2.84 No history, meds, or risk factors. Pattern looked to be BER. mm in V2 and 4.08
It tells us there is an active, ongoing process — and that prompt cath with acute reperfusion is likely to be needed regardless of whether or not the millimeter-definition of a STEMI has been satisfied. A cknowledgment : My appreciation to 張三毛 = JJ ( from Taiwan ) for the case and this tracing. =
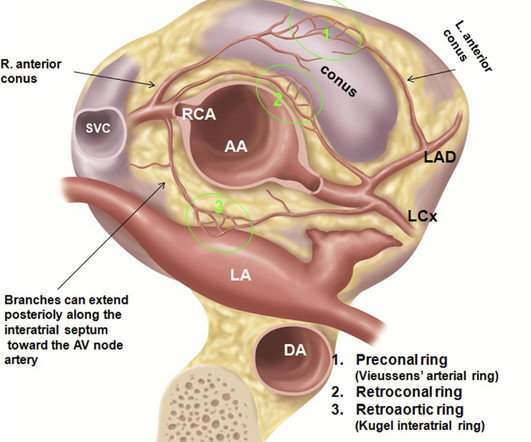
2017 ) Clinical implication of such coronary anomalies Apart from angiographic surprises, these anomalous coronary arteries may under-perfuse the ventricle and present as unexplained cardiomyopathy , until we realize the anatomical errors in coronary anatomy. We know, how adverse is the outcome of Left main STEMI. Annu Rev Physiol.
He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size. The anatomy and lead placement create very small voltage compared to the other main coronary distributions. EF was 55%.
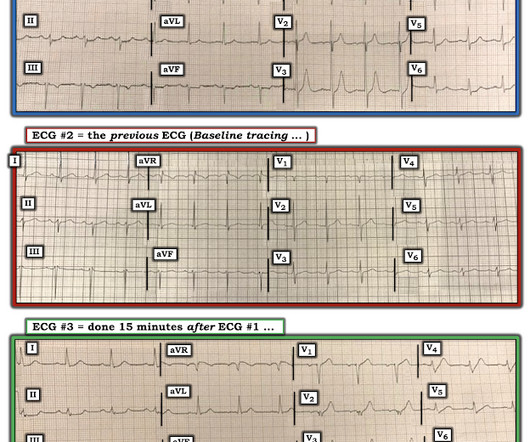
Some patients will not progress (or not as quickly) to obvious STEMI, as in this case. P EARL — One of the best ways to hone your ECG interpretation skills — is by r etrospective r eview of s erial t racings on cases in which you know the anatomy. Sometimes serial ECGs minimizes the delay.
90% stenosis of the proximal ramus intermedius, pre procedure TIMI II flow The ramus intermedius is a normal variant on coronary anatomy that arises between the LAD and LCX. Recall that air is a poor conductor of electricity and will, therefore, generate smaller amplitudes on posterior leads (hence why STEMI criteria requires only >0.5
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. Here is his angiogram: This shot shows that the left circumflex (LCx) is occluded at the ostium (origin). This is seen just millimeters beyond the tip of the catheter. The patient recovered well.
This can only be due to STEMI. Initial priorities in this patient were clearly to determine the anatomy — and reestablish coronary perfusion. However, cardiogenic shock usually takes some time to develop, so it is probably subacute." Then I was told that the troponin I returned at greater than 50,000 ng/L.
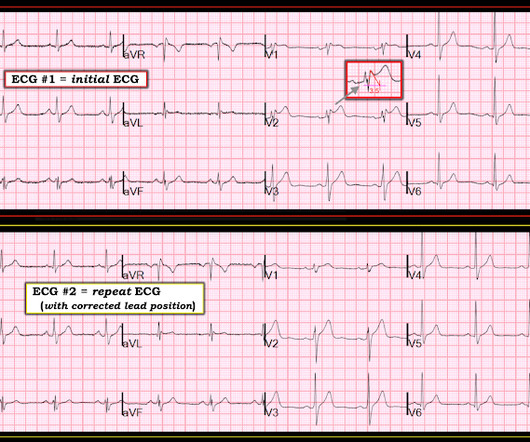
Saddleback ST Elevation is almost never STEMI 2. An inverted P-wave in lead V2 implies lead misplacement too high Saddleback in STEMI: Here are the only 2 ECGs with V2 "saddleback" that I have ever seen which really represented an LAD Occlusion: Anatomy of a Missed LAD Occlusion (classified as a NonSTEMI) A Very Subtle LAD Occlusion.T-wave
Time window s for intervention for thrombolysis in STEMI starts from onset of chest pain, but when it comes to primary PCI, a different time window takes the center stage pushing the former to the background. How can we have uniform std of 90-120 minutes D2B in all STEMI cases ? Why is this disparity?
There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. The case was reviewed by all parties, and it was stated correctly that the ECG does not meet the STEMI criteria. The STEMI vs. NSTEMI paradigm is not the best way to decide who needs emergent reperfusion therapy.
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. 24 yo woman with chest pain: Is this STEMI? This is not "diffuse", this is simply anterior, lateral, and likely apical.
First in slow motion with a freeze frame with annotated vessel anatomy, then at normal speed. Limitations of registry data: This patient presented with STEMI (-) OMI and developed STEMI the following day. In the world of STEMI, we are incapable of recognizing the first ECG as a false negative. Angiogram is shown below.
Note: the 2022 ACC Expert consensus Chest pain guidelines state that "posterior STEMI-Equivalent" is a sign of acute coronary occlusion. 2/3 of STEMI have a peak 4th generation troponin I greater than 10.0 Comment: The first ECG is diagnostic of OMI that does not meet STEMI criteria. NSTEMI-OMI").
The fear comes built in with the diagnosis often amplified by young felllows on call (& often times by senior consultants as well) It may appear real, from a clinical angle, but trust, when we deal with the whole gamut of so-called ACS (other than STEMI), there is indeed a benign face in many of them.
The first EKG was concerning for a Wellen’s-like pattern of subtle reperfusion changes in the setting of stuttering anginal-equivalent symptoms, but none were diagnostic of STEMI or OMI. Later in the night, the patient became bradycardic and developed a Mobitz II pattern , but he remained asymptomatic and hemodynamically stable.
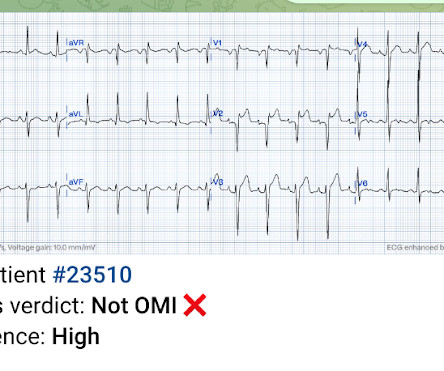
Queen : she saw no OMI (no "STEMI Equivalent") either Continued : Now, she says she was walking to the bathroom when she experienced acute onset substernal chest pressure radiating into her neck and left arm. Her ECG afterward is shown below: ECG from five days prior Smith : this shows an old inferior MI with persistent ST elevation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content