This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
If you understand the pericardial anatomy fully, you can call yourself real master of clinical anatomy. Inflammatory pericarditis can occur in differential fashion. For example, the most common chronic pericarditis tuberculosis affects the fibrinous layer. Post MI pericarditis involves the epicardium. 2020.01.009.
Pericarditis is rare — but myocarditis is not , so especially in this age group — more information is needed to quickly determine if this could be an acute MI, myocarditis, or none of the above.
To revise the anatomy lessons, this is the external jugular vein and this is the internal jugular vein. That occurs in right heart failure and constrictive pericarditis. Constrictive pericarditis is an important cause for Kussmaul sign or inspiratory increase in jugular venous pressure.
Pericarditis? For coronary anatomy, see here: [link] This is the post intervention ECG: All ST Elevation is gone (more proof that it was all a result of ischemia) Formal Echo: Normal estimated left ventricular ejection fraction - 55%. Time zero What do you think? There is inferior ST elevation. Is it normal variant? It was stented.
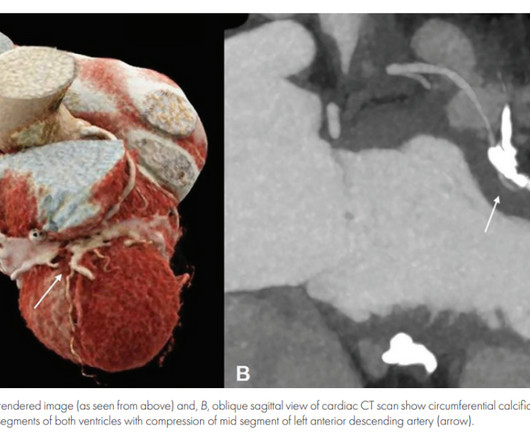
Pericarditis? These include coronary artery spasm ( as may occur from cocaine use or binge alcohol drinking ) — myocardial bridging ( that may be the cause of intermittent acute ischemia ) — aberrant anatomy of a coronary artery ( which may present with sudden rupture causing acute infarction or sudden death at any age! ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content