This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. 2000;139:430–436. Am J Cardiol.
Hyperacute T Wave in the Early Diagnosis of Acute MyocardialInfarction. Interpretation of acute myocardialinfarction with persistent “hyperacute T waves” by cardiac magnetic resonance. High T waves in the earliest stage of myocardialinfarction. Prompt cath to define the anatomy should be expedited.
These advancements included identifying cardiac anatomy, measuring myocardial mass and chamber sizes, quantifying blood flow, and characterizing tissue properties using different relaxation times and gadolinium contrast. The third stage, beginning in 2010 and continuing today, emphasized the widespread clinical use of CMR.
Intra-procedural data included access route, coronary anatomy, lesion complexity, number of stents deployed, door-to-balloon time for primary PCI, and any intra-procedural complications. Pre-procedural data included patients’ baseline characteristics (age, gender, clinical presentation and comorbidities).
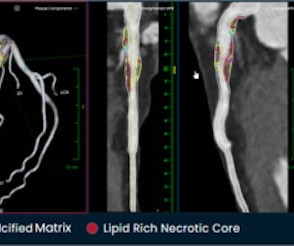
tim.hodson Tue, 10/01/2024 - 10:50 PHOTO CAPTION: The Elucid PlaqueIQ user interface is a fully interactive visualization of the patient’s coronary anatomy, showing specific plaque type and amount across various views to inform physician assessment of risk and patient-specific treatment pathway.
Although not striking, this is clearly a diagnostic ECG for infero"posterior" myocardialinfarction due to coronary occlusion (OMI), most likely due to left circumflex (LCx) artery occlusion. mm STE even in the fourth universal definition of myocardialinfarction. Considerations on the naming of myocardialinfarctions.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chest pain to Dr. McLaren. Incidence of an acute coronary occlusion. Am J Med 2019, 132(5):622-630. Miranda DF, Lobo AS, Walsh B, et al.
The STEMI guidelines do state that hyperacute T-waves "may indicate early acute myocardialinfarction" but do not discuss it as a "STEMI equivalent." The finding of de Winter T waves in both inferior and anterior lead locations is consistent with likely LAD wraparound anatomy.
Thin posterior wall in inferior wall myocardialinfarction causing abnormal septal to posterior wall ratio can also cause suspicion of ASH. Evaluation of diastolic characteristics of LV and LV and coronary anatomy evaluation are other diagnostic uses of cath in HCM. The role of cath now a days is mostly for septal ablation.
Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion MyocardialInfarction (Versus Nonocclusive Ischemia). 90% stenosis of the proximal ramus intermedius, pre procedure TIMI II flow The ramus intermedius is a normal variant on coronary anatomy that arises between the LAD and LCX.
The anatomy and lead placement create very small voltage compared to the other main coronary distributions. Diagnosis of acute myocardialinfarction in angiographically documented occluded infarct vessel: limitations of ST-segment elevation in standard and extended ECG leads. EF was 55%. From AM et al.
mg tablet), ananti-inflammatory atheroprotective cardiovascular treatment, to reduce the risk of myocardialinfarction (MI), stroke, coronary revascularization, and cardiovascular death in adult patients with established atherosclerotic disease or with multiple risk factors for cardiovascular disease.
mg tablet), ananti-inflammatory atheroprotective cardiovascular treatment, to reduce the risk of myocardialinfarction (MI), stroke, coronary revascularization, and cardiovascular death in adult patients with established atherosclerotic disease or with multiple risk factors for cardiovascular disease.
Without oxygen, the cells would quickly die, leading to a heart attack (myocardialinfarction). MyocardialInfarction (Heart Attack) : A heart attack occurs when blood flow to part of the heart is blocked, causing damage to the heart muscle. CAD is one of the leading causes of heart attacks.
The long-term prognostic relevance of post-PCI myocardial injury remains uncertain.METHODS:Consecutive adults aged 18 years with stable ischemic heart disease who underwent elective PCI at NYU Langone Health between 2011 and 2020 were included in a retrospective, observational study.
Angiogram: --"Suspected culprit for the patient's non-ST elevation myocardialinfarction with refractory chest discomfort (although it had resolved prior to arrival to the cardiac catheterization lab), is a ruptured plaque in the distal circumflex with local embolic occlusion of the distal OM 3."
First in slow motion with a freeze frame with annotated vessel anatomy, then at normal speed. Who seriously believes that the portion of myocardium that infarcted did not matter? How is a patient permitted to infarct his inferior wall in a cath capable facility while being monitored for known myocardialinfarction.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content