
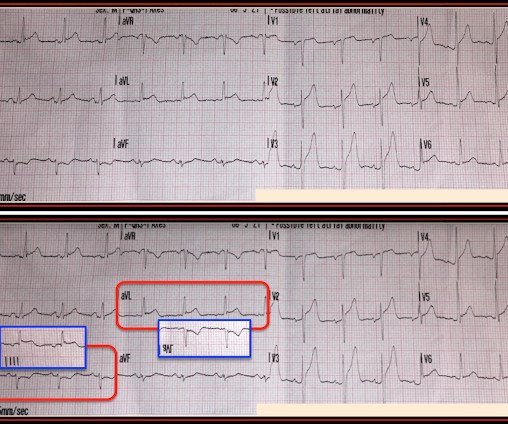
Chest pain and new regional/reciprocal ECG changes compared to previous ECGs: code STEMI?
Dr. Smith's ECG Blog
NOVEMBER 27, 2023
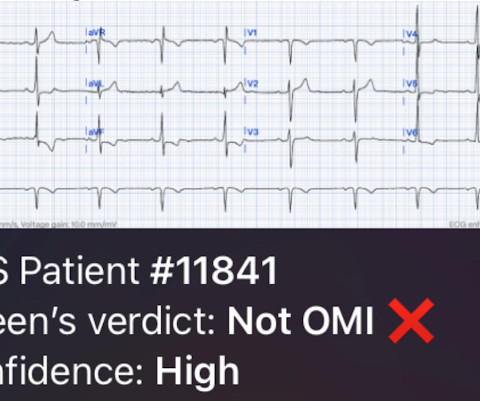
The admission and discharge diagnosis both attributed the ECG changes and echo findings to ischemia. The biggest problem with STEMI criteria are false negatives – because this costs patient’s myocardium, with greater mortality and morbidity. baseline ECGs may fluctuate over time, and not necessarily represent dynamic ischemia 4.


















Let's personalize your content