This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
ObjectiveSpinal cord ischemia due to damage or occlusion of the orifices of aortic segmental arteries (ASA) is a serious complication of open and endovascular aortic repair.
Coronary anatomy and SYNTAX(Synergy between percutaneous coronary intervention with Taxus and cardiac surgery) scores were measured using coronary computed tomography angiography. BACKGROUND:The appropriate use criteria for revascularization of stable ischemic heart disease have not been evaluated using randomized data.
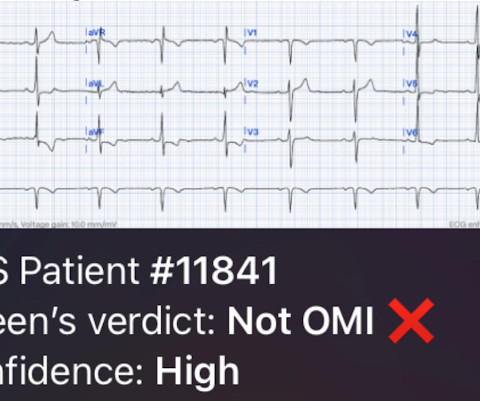
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiac arrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). To EMPHASIZE: This pattern of diffuse Subendocardial Ischemia does not suggest acute coronary occlusion ( ie, it is not the pattern of an acute MI ).
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. Ischemia can be disguised by a wide escape rhythm, which decreases the sensitivity of ECG.
The Shockwave E 8 catheter is designed to optimize the treatment of patients with calcified femoro-popliteal and below-the-knee peripheral artery disease (PAD), including patients with complex chronic limb-threatening ischemia (CLTI). PAD affects more than eight million people aged 40 and older in the United States.
The admission and discharge diagnosis both attributed the ECG changes and echo findings to ischemia. baseline ECGs may fluctuate over time, and not necessarily represent dynamic ischemia 4. Below is the discharge ECG, which showed the baseline ECG without any reperfusion T wave inversion. Take home 1. GREAT case by Dr. McLaren!
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chest pain to Dr. McLaren. His response: “subendocardial ischemia. A emergent cardiology consult can be helpful for equivocal cases.
Which of the vessels likely provides blood supply to the circled area in the below polar plot image in a patient with normal coronary anatomy? The images demonstrate a moderately extensive, mildly severe reversible defect in the mid and distal anterior/anterolateral wall consistent with ischemia. The technologist performs a MUGA scan.
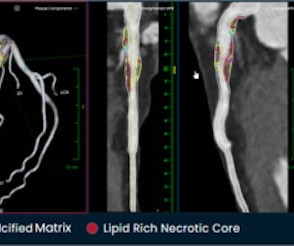
tim.hodson Tue, 10/01/2024 - 10:50 PHOTO CAPTION: The Elucid PlaqueIQ user interface is a fully interactive visualization of the patient’s coronary anatomy, showing specific plaque type and amount across various views to inform physician assessment of risk and patient-specific treatment pathway. Cardiovasc. 6 (3) (2019).
Shark Fin" ST segment elevation is most often a sign of severe transmural ischemia that results from acute coronary occlusion. Consideration of prompt cardiac cath is essential for clarifying the anatomy — since in many ( most ) cases, prognosis is likely to be poor unless there is prompt reperfusion. (
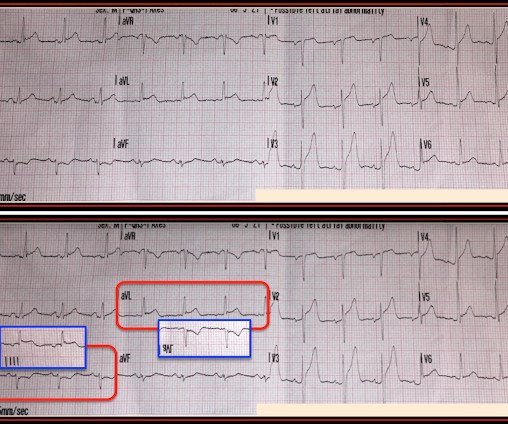
This qualifies as " dynamic " ST-T wave change — and in a patient with new chest pain, this is indication for prompt cath to define the anatomy and ensure reperfusion. ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ).
For example, inferior OMI with concomitant critical stenosis produces a combined pattern ( Aslanger’s pattern ) with inferior STE and subendocardial ischemia · occlusion of two infarct-related arteries simultaneously ("co-culprits") In this case there were two infarct-related arteries.
For coronary anatomy, see here: [link] This is the post intervention ECG: All ST Elevation is gone (more proof that it was all a result of ischemia) Formal Echo: Normal estimated left ventricular ejection fraction - 55%. More likely, these T waves probably reflect ischemia of uncertain age. It was stented.
Ongoing ischemia (by symptoms, ECG, or troponin) despite maximal medical management is an indication for emergent cath lab activation. == MY Comment by K EN G RAUER, MD ( 8/15/2019 ): == Once again, the w rong q uestion was a sked in this case. Any Q-wave in V2 in the presence of an otherwise normal QRS complex is abnormal.
This is ischemia until proven otherwise. A fixed stenosis in that other artery, especially in the context of hypotension from the occlusion of the first coronary artery, can lead to ischemia and very poor LV function and worsening shock. I learned that the patient is on Sotalol for control of PVCs. This explains the long QT.
ACTUAL CORONARY ANATOMY: Dominance: Right LM: A 5 mm vessel which bifurcates into the LAD and LCx coronary artery. 2) There are three causes of tall T waves; hyperkalemia, hyperacute ischemia and normal variant (Atlas of Electrocardiography by K. Wang, (pages 222-224). Wang, page 171).
Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia). 90% stenosis of the proximal ramus intermedius, pre procedure TIMI II flow The ramus intermedius is a normal variant on coronary anatomy that arises between the LAD and LCX.
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia). The patient recovered well. J Am Heart Assoc.
If the patient had been "lucky," his symptoms from the prior day might have been due to ischemia prolonged and intense enough to result in small troponin increase. The anatomy and lead placement create very small voltage compared to the other main coronary distributions. EF was 55%. The patient did well at least in the short term.
This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. Coronary Artery Disease (CAD) CAD, which involves the narrowing or blockage of coronary arteries due to plaque buildup, can reduce blood flow to the heart.
These include coronary artery spasm ( as may be precipitated by cocaine use or binge alcohol drinking ) — myocardial bridging ( that may be the cause of intermittent acute ischemia ) — aberrant anatomy of a coronary artery ( which may present with sudden rupture causing acute infarction or sudden death at any age! ).
Session 510) To Treat or Not to Treat Anatomy and Ischemia? (Session 508) Battle of the Imagers - Jeopardy Edition! Session 509) Who Wants to Be a Millionaire in Eradicating Vascular Medicine Disparities?
Additionally, the heart’s high demand for oxygen makes it particularly vulnerable to conditions like ischemia (reduced blood flow), which can weaken or damage the heart muscle if left untreated. Common Problems in Coronary Circulation Understanding coronary circulation helps shed light on common heart conditions.
This ECG is all but diagnostic of subepicardial ischemia of the anterior, lateral, and inferior walls, most likely due to Occlusion MI (OMI), probably of the LAD. because if it does, then urgent cath to define the anatomy is clearly indicated. Here is his ECG on arrival: What do you think? Leads II and aVF also have hyperacute T-waves.
These include coronary artery spasm ( as may occur from cocaine use or binge alcohol drinking ) — myocardial bridging ( that may be the cause of intermittent acute ischemia ) — aberrant anatomy of a coronary artery ( which may present with sudden rupture causing acute infarction or sudden death at any age! ).
We know, stress tests can give false positive results suggesting ischemia in at least 20% of patients for various reasons. We are obsessed with anatomy. Our flawed intellect keeps asking this question: How can I trust physiology (Flow) without documenting a good anatomy? In fact, truth is the other way around.
Given the right coronary anatomy seen during angiography, it is particularly interesting that subtle T wave changes were seen on the previous EKGs in the high lateral leads that would otherwise only be expected with a more proximal RCA lesion. Also: electrical instability, pulmonary edema, or hypotension.
That said there were no clinical symptoms or ECG findings suggestive of ongoing ischemia. You have given IV MgSO4 a fast acting -blocker and IV amiodarone bolus and infusion. The possibility of an ischemic cause of the ventricular arrhythmia has to be considered! Troponin T was negative on admission and on repeat blood draw.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content