This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
1 Factors related to congenital heart disease, such as underlying anatomy, surgical repair technique and scars, can all be considered as AA substrates. Early diagnosis and ECG documentation is therefore essential for arrhythmia management. Of these, AA is one of the leading causes for hospital admissions in ACHD care.
While CT-guided CNA's feasibility is documented, data about GP anatomy and comprehensive evaluations of GP targeting methods remain scarce. Cardioneuroablation (CNA) targets ganglionated plexus (GP) to treat neurally-mediated syncope, yet a standardized GP identification method is lacking.
The primary reason is, the LV epicardial lead pacing site was pre-selected by the coronary sinus anatomy. This weeks JAMA has reported an encouraging results with this device.The study documented reduction in end systolic volume by 16% and the ejection fraction as well. Red 1) What about totally leadless CRT ?
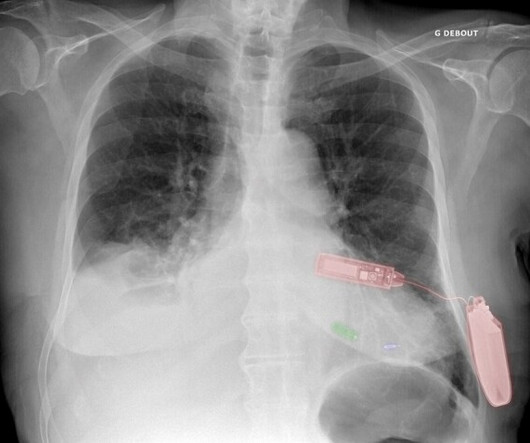
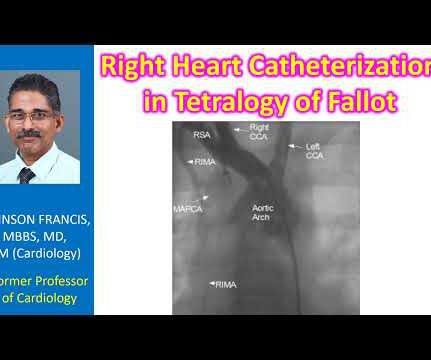
Diagnostic cardiac catheterization may be needed especially in tetralogy of Fallot with pulmonary atresia, to assess the pulmonary anatomy, including size and distribution of peripheral pulmonary arteries. Magnetic resonance imaging is another way of documenting coronary anomalies. If McGoon’s ratio is below 0.8,
Freedom from documented atrial arrhythmia recurrence at 12 months was 79.9% (AF 82.7%, AFL 96.5%, AT 98.1%), antiarrhythmic drugs (AAD) were continued or re-initiated in 26.8% Freedom from documented recurrence at 12 months in these pts was 82.0%. of patients after the 3-month blanking period.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. His unique cath film demonstration removes all doubt about the anatomy — with the clearest illustration of acute septal perforator occlusion that I have seen!
Degree of outflow obstruction can be documented along with the classical Brockenbrough-Braunwald-Morrow sign. Evaluation of diastolic characteristics of LV and LV and coronary anatomy evaluation are other diagnostic uses of cath in HCM. The sign is an increased LVOT gradient after a ventricular premature complex.
For coronary anatomy, see here: [link] This is the post intervention ECG: All ST Elevation is gone (more proof that it was all a result of ischemia) Formal Echo: Normal estimated left ventricular ejection fraction - 55%. In other words, inferior MI with some posterior involvement). It was stented.
A brief history of NAFLD and NASH The field of hepatology has struggled to come up with adequate nomenclature for liver disease since one of the most important figures in historical pathological anatomy, Carl von Rokitansky, documented visceral and subcutaneous adiposity in overfed children in 1849.
second that might document underlying SSS. This is because of “the great variation in anatomy and pathology producing this pattern” — as well as the fact that one will usually not be able to make a definitive diagnosis of trifascicular block from the surface ECG.
The anatomy and lead placement create very small voltage compared to the other main coronary distributions. Diagnosis of acute myocardial infarction in angiographically documented occluded infarct vessel: limitations of ST-segment elevation in standard and extended ECG leads. EF was 55%. The patient did well at least in the short term.
The purpose of the document was to consolidate multiple terms and provide clear definitions for terms applicable to cardiac CT. The document underwent organizational review by the SCCT Board of Directors and the AAPM board, as well as the ACR, NASCI and RSNA’s boards, in addition to peer reviewers.
We are obsessed with anatomy. Our flawed intellect keeps asking this question: How can I trust physiology (Flow) without documenting a good anatomy? A good epicardial anatomy rarely guarantee good physiology. (It Final message Most of us (Cardiologists) find it difficult to trust physiology, ie excercise capcity.
There is very scarce documentation, but the next ECG was obtained around 1 PM. First in slow motion with a freeze frame with annotated vessel anatomy, then at normal speed. Documentation regarding the severity of this patient's CP remained "scarce" without any correlation of CP severity to the repeat ECG that was finally done.
Documentation does not indicate whether she had persistent chest pain during this time. LAO cranial shot of the RCA Here is an annotated still showing anatomy: Dotted black lines indicate filling defects due to thrombus: The cath report described mostly organized thrombus and heavy thrombotic burden. No repeat ECGs were obtained.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content