This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
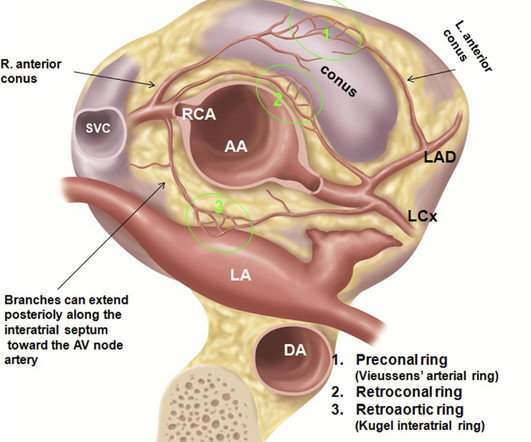
2017 ) Clinical implication of such coronary anomalies Apart from angiographic surprises, these anomalous coronary arteries may under-perfuse the ventricle and present as unexplained cardiomyopathy , until we realize the anatomical errors in coronaryanatomy. Annu Rev Physiol. Some unanswered queries 1.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chest pain to Dr. McLaren. All electrocardiograms (ECGs) and coronaryangiograms were blindly analyzed by experienced cardiologists.
Young people can suffer acute coronary occlusion, whether by typical atherosclerotic plaque rupture, or by coronary anomalies, coronary aneurysms, dissections, spasm, etc. The wall motion abnormalities of Takotsubo cardiomyopathy and LAD OMI can be similar.
Mostly, you can’t escape from a coronaryangiogram” Next option is CT angiogram, Thallium or dobutamine stress. Out of 5 cardiologists I consulted, 4 asked me to go for an immediate angiogram. We are obsessed with anatomy. A good epicardial anatomy rarely guarantee good physiology. (It
Strangely, we are also taught , “No ACS should be considered benign, until you see the coronaryanatomy” I wish patients realise, how difficult it is to practice cardiology, for that matter any field of emergency medicine. You can’t err at the same time , you are not supposed to treat inappropriate as well.
CT coronaryangiogram showed a hypoplastic RCA and dominant LCx. Figure-5: Long lead II recording on oral flecainide ( 10 minutes of continuous recording each line being 1-minute long ). No PVCs are seen. A workup was undertaken in search of a cause of the patient's ventricular arrhythmia. There were no plaques or stenoses.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content