This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think?
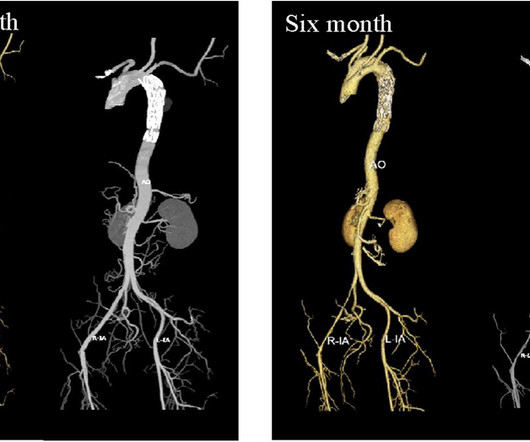
Follow-up CTA scans at one- and six-month post-operation showed that the aortic stent was well-positioned, with no visible primary lesion. After a comprehensive, multidimensional evaluation of the patient's medical history, CTA, and esophagography, we successfully performed TEVAR procedure.
There is new data showing better outcomes when bystander lesions (non-culprit) are stented. == MY Comment by K EN G RAUER, MD ( 8/28/2020 ): == Dr. Smith highlights a number of important lessons to be learned from today’s case. Initial priorities in this patient were clearly to determine the anatomy — and reestablish coronary perfusion.
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chestpain that started while mowing the lawn. The LAD lesion was acute and required 3 stents to restore flow. Here is his ECG on arrival: What do you think?
Written by Pendell Meyers A male in his early 50s presented with waxing and waning chestpain starting at rest. Although I do not see much difference between the ECGs, for some reason (perhaps ongoing pain or rising troponins) the case was reevaluated at this time and the decision was made to perform cath.
60-something with h/o MI and stents presented with chestpain radiating to the back and nausea/vomiting. It was stented. The patient had a p rior h istory of MI + stents. Time zero What do you think? There is inferior ST elevation. Is it normal variant? Is it ischemic (OMI)? Pericarditis?
Case A 39-year-old male without prior medical history presents with chestpain that started 2 hours prior to presentation. He says that the pain intensity was 10/10 at home but now about 4/10. Despite the clinical stability and decreasing pain, this patient needs an immediate angiogram. Here are his publications.)
Written by Willy Frick A young woman with a history of paroxysmal nocturnal hemoglobinuria presented with acute substernal chestpain. The report describes heavy plaque in the proximal RCA by IVUS, but no lesions in the previously occluded RPL branch and no stent was deployed. < < 35) and rose overnight to 4951.
A 50 something male presented in the evening to ED for evaluation of chestpain that started at 1600. He reports this was similar to how he felt when he had his heart attack 4 years prior, now s/p 4 stents. The chestpain continued for hours. The patient was still having chestpain.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content