

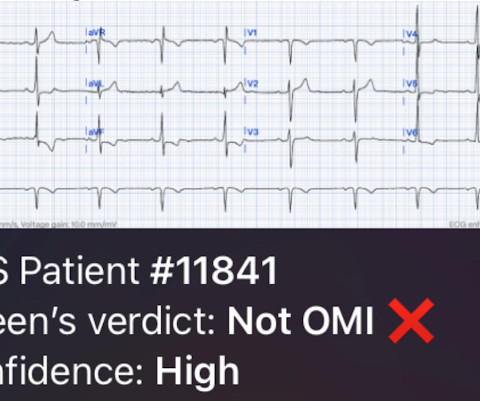
ECG Blog #448 — A Young Man with Chest Pain.
Ken Grauer, MD
SEPTEMBER 21, 2024
For example, considering whatever symptoms that the patient may have had ( ie, chest pain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. STEP #2 = Clinical Impression — in which we correlate our assessment that we made in Step #1 to the clinical situation at hand.




















Let's personalize your content