This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
When left untreated, arrhythmias may significantly increase the risk of stroke, heart failure, and sudden cardiacarrest. With unmatched accuracy, we can tailor treatments to each patient's unique anatomy, enhancing safety and efficacy.” “We
About 45 minutes after the second EKG, the patient was found in cardiacarrest. Later the next day, she went into cardiacarrest again. By the time I saw the repeat EKG, the patient was already in cardiacarrest. Prompt cath to define the anatomy should be expedited. She could not be resuscitated.
CardiacArrest or Sudden Death: Cardiomegaly increases the risk of life-threatening arrhythmias, which can cause sudden cardiacarrest. Blood Clots: An enlarged heart is more prone to developing blood clots, which can lead to stroke or pulmonary embolism.
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiacarrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). Given this situation — the anatomy needs to be defined to determine if acute reperfusion with PCI will be needed to prevent imminent coronary occlusion. =
Expert ECG interpretation could have prevented this man's cardiacarrest, and almost certainly would have resulted in a much smaller MI and therefore better long term prognosis. because if it does, then urgent cath to define the anatomy is clearly indicated. Somewhere along the way the initial ECG was misinterpreted.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chest pain to Dr. McLaren. Thirty-six patients (36%) presented with cardiacarrest, and 78% (28/36) underwent emergent angiography.
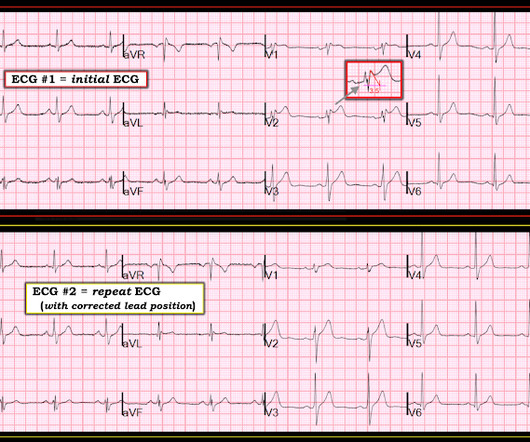
An inverted P-wave in lead V2 implies lead misplacement too high Saddleback in STEMI: Here are the only 2 ECGs with V2 "saddleback" that I have ever seen which really represented an LAD Occlusion: Anatomy of a Missed LAD Occlusion (classified as a NonSTEMI) A Very Subtle LAD Occlusion.T-wave wave in V1??
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content