This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Description : Regular Wide Complex Tachycardia at a rate of about 160. SVT with aberrancy?
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
PEARL # 2: When the rate of AFib is rapid — this irregular tachycardia may look regular when it is not. That the rhythm is AFib — is easier to appreciate in Figure-3. Clearly, the rhythm is AFib — here with a controlled ventricular response. Figure-3: Today's rhythm is not regular ( See text ).
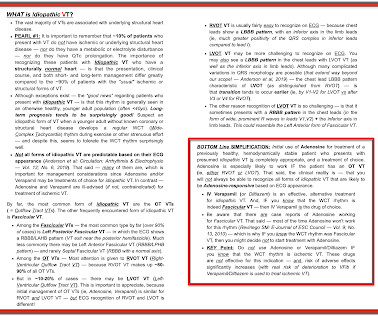
The 2019 ESC Guidelines for the management of patients with supraventricular tachycardia indicated that IV Amiodarone should not be considered in these populations. KEY Point: Nothing other than AFib with WPW results in a ventricular response this fast ( which is why Figure-2 is pathognomonic for AFib in a patient with WPW ).
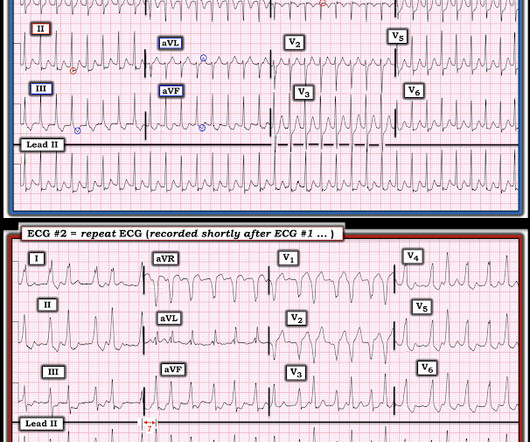
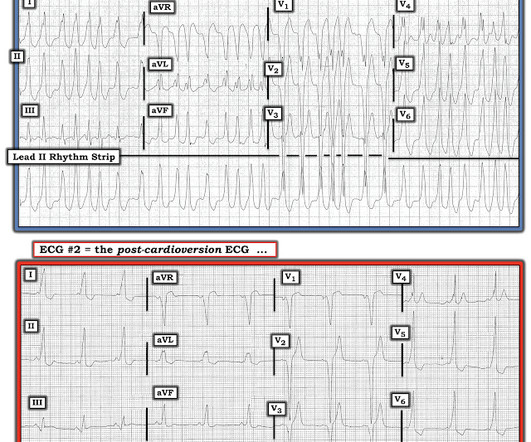
The two ECGs above were texted to me with the text: "Young Guy came in in SVT but now in and out of irregular wide complex tachycardia. -- not sure if polymorphic VT vs. a fib with WPW." FINAL Points in Today's CASE: Even though the SPERRI value during AFib in today's case was not below 250 msec. Definitely atrial fibrillation.
Detection of Irregular Heart Rhythms Devices such as the Apple Watch or Fitbit Sense can detect irregular heart rhythms, including atrial fibrillation (AFib). These early warnings are critical, as AFib increases the risk of stroke and other heart-related complications.
Wide-complex tachycardia: VT or aberrant, or "other?" A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. Sinus tachycardia with aberrancy was unlikely as the rate was consistently 150 bpm, without spontaneous variation. And indeed the QRS morphology strongly supported VT (e.g.
His previous echo one month prior shows the same thing: “consistent with old infarct in LAD vascular territory, with EF 45%” "I think there is something else causing his tachycardia which is exaggerating his EKG findings and mimicking an acute myocardial infarction." The patient spontaneously converted back to sinus tachycardia.
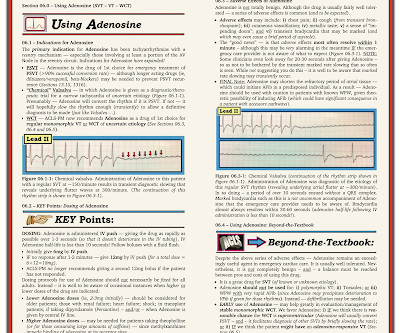
There is a regular wide complex tachycardia. Remember : Adenosine is safe in Regular Wide Complex Tachycardia. Rather, from this one: Very Fast Very Wide Complex Tachycardia Ideally, one would cardiovert. At the time, it seemed that virtually all cardiac patients with chronic AFib or heart failure were on this medication.
There were times when it would be usurped by sinus tachycardia, then return to this rhythm. This does NOT seem irregularly irregular enough for AFib … Instead — there is almost “group beating” with “Wenckebach periodicity”. CT of chest showed the bullet path through his right lung but nowhere near his heart. There is a wide complex.
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Is longterm endurance-training a risk factor for AFib and AFlutter? == Why is Today's Initial Rhythm AFlutter? Sinus tachycardia does not go this fast.
Or are they due to ventricular tachycardia (VT). Within about an hour, he spontaneously converted to sinus rhythm: == My Comment by K EN G RAUER, MD ( 4/23/2019 ): == Interesting rhythm — in which the tachycardia alternates from a wide to narrow QRS complex. There are no P-waves. Sinus P waves are absent.
Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered. Nevertheless, the widths of both the QRS complex and the RS duration are similar in both the old ECG and the tachycardia.
Multifocal Atrial Tachycardia 2. AFib is the irregularly irregular rhythm that is most commonly confused with MAT — and , AFib is much, much, much more common than true MAT. The rhythm is indeed irregularly irregular, so atrial fibrillation must be considered. Sinus with multifocal PACs 3. Sinus with multifocal PVCs 4.
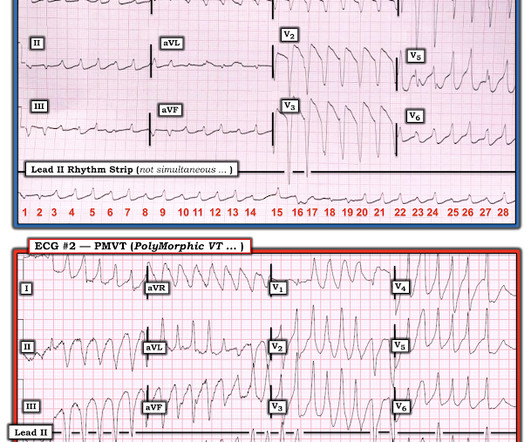
MY THOUGHTS on ECG #1: My initial impression on looking at the ECG in Figure-1 — was that the rhythm was either rapid AFib in a patient with WPW — or — PMVT ( P oly M orphic VT ). The reason I initially thought the underlying rhythm was AFib — is that no atrial activity is seen in any lead and the rhythm “looks” irregular. See text ).
Therefore — the rhythm in ECG #1 is almost certain to be AFib ( A trial F ibrillation ) , seen here with a “rapid” ventricular response. Under normal conditions with AFib — the refractory period of the AV node does not allow more than 150-to-200 impulses/minute to be conducted to the ventricles.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ). Sinus Tachycardia ( common in any trauma patient. ).
The finding of a fairly regular, wide tachycardia without clear sign of atrial activity ( especially when seen in an acutely symptomatic patient ) — should immediately prompt a diagnosis of VT until proven otherwise. These findings suggest that instead of VT — the rhythm in Figure-1 is AFib with a fairly rapid ventricular response.
Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia. Ventricular tachycardia – more than 7 consecutive complexes originating from ventricles at a rate of > 100 bpm. Supraventricular tachycardia – more than 7 consecutive complexes of supraventricular beats at a rate of > 100 bpm.
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( How would YOU interpret this tracing? How to manage the patient?
Because of this, it is uncommon to see sinus tachycardia with a prolonged PR interval. And I wish I had record of ECG monitoring just before — and during — and just after the rhythm changes from the regular tachycardia in ECG #1 — to the bigeminal rhythm in ECG #2. This is precisely what we see in Figure-6.
Many patients have a T achy- B rady syndrome in which tachyarrhythmias ( most commonly rapid AFib ) alternate with periods of bradycardia. Because the SA node is sick the SA node recovery time is often prolonged, which is why long pauses most commonly follow episodes of tachycardia ( which produced SA node suppression ).
The ECG there reportedly showed an irregular tachycardia, and the patient was immediately referred to the emergency room. Here is her ECG on arrival: There is a wide complex tachycardia that is irregularly irregular (this is difficult to determine at these very high rates). Vitals were within normal limits other than heart rate.
The presence or absence of five predetermined cardiac arrhythmias were evaluated: atrial fibrillation/flutter (AFIB), ventricular bigeminy, ventricular trigeminy, ventricular tachycardia (VT), and high-grade atrioventricular block (AVB).Results:The For AFIB, the sensitivity was 0.76 for the AI platform compared to 0.74
I was sent the ECG shown in Figure-1 — being told only that providers on the case suspected AFib ( A trial Fib rillation ) with RBBB ( R ight B undle B ranch B lock ) aberrancy. QUESTIONS: Is the wide tachycardia that is seen best in the chest leads, too irregular to be VT ( V entricular T achycardia )? —
Electrical cardioversion may be recommended for you if you have certain types of arrhythmias, such as: Atrial fibrillation (AFib): This is the most common type of arrhythmia, and it can cause symptoms like dizziness, fatigue, and difficulty breathing. Atrial flutter: This is a rapid but regular heart rhythm often progressing to AFib.
ACUTE MI (I allowed Acute MI to be in the report because I knew there would be an elevated troponin from ischemia, which is the definition of acute MI -- but in this case it would most likely be a Type 2 MI from tachycardia) There is also LA-RA lead reversal. The rhythm is rapid AFib. The QRS complex in lead I looks "funny".
ECG Blog #71 — Regarding the Ashman Phenomenon with AFib. The September 30, 2019 post in Dr. Smith’s ECG Blog — for an example of “MAT”, but without the tachycardia. ( And why the most common form of aberrant conduction manifests RBBB morphology ). ECG Blog #70 — Reviews the A shman P henomenon ( re aberrant conduction ).
Among the fast Supraventricular Rhythms: This is not AFib — because the rhythm is regular. P utting I t A ll T ogether : — The Rhythm in Figure-1 What we have just described is the following: A regular WCT ( = W ide- C omplex T achycardia ) at a rate very close to 300/minute — without clear sign of atrial activity.
With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Systematic Assessment of the ECG in Figure-1: My Descriptive Analysis of ECG findings in Figure-1 is as follows: Sinus tachycardia at ~110/minute. The patient had mild but diffuse abdominal tenderness.
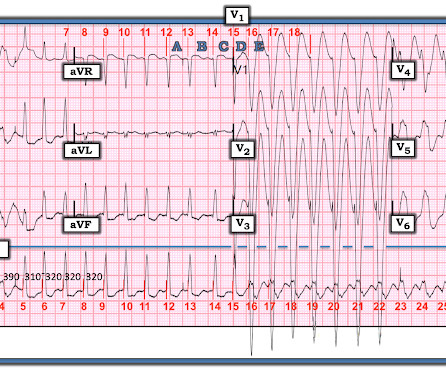
But there are 3 other wide beats in the tachycardia that begins with beat #6 ( = beats #7; 13,14 ). Similar-looking wide beats #7,13,14 must also be aberrantly conducted supraventricular impulses — and since P waves are lost after beat #6 and subsequent R-R intervals are irregular — beats #7-thru-16 constitute a run of rapid AFib.
Sinus Tachycardia ( common in any trauma patient. ). Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). RBBB ( as by far the most common conduction defect — owing to the more vulnerable anatomic location of the RV ).
The combined solutions are expected to enhance performance and streamline workflows for electrophysiologists during catheter ablation procedures to treat atrial fibrillation , AFib. 1 Approximately 33 million patients worldwide are living with AFib. 1 Approximately 33 million patients worldwide are living with AFib.
space-line Alcohol and ‘Holiday Heart Syndrome’ Holiday heart syndrome refers to episodes of supraventricular tachycardia: a sudden arrhythmia or irregularity in which the heart beats much faster than normal, explains Dr. Schuitema. Alcohol acts as a natural irritant to the heart muscle, says Dr. Tarditi.
Initial vital signs include: NIBP 99/58 HR 150-160 (trend) RR 10 (spontaneous, but shallow) SpO2 86 (RA) BBS CTA The initial rhythm strip is attached: Figure 1 There is a wide complex tachycardia of varying morphology, amplitude, and R-R cycle length. The rS configuration in Lead I displays a persistent rightward axis.
2) Tachycardia to this degree can cause ST segment changes in several ways. First , there can simply be diffuse ST depressions (which obligates reciprocal STE in aVR) associated with tachycardia which are not indicative of ischemia. Sometimes you must correct the rhythm to see what lies underneath. Is this inferor STEMI?
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. An ECG was recorded: This shows a regular narrow complex tachycardia at a rate of about 160. See my quick review of atrial tachycardia below) The tachycardia spontaneously resolved. BP:143/99, Pulse 109, Temp 37.2 °C
The team immediately paged cardiology, concerned for polymorphic ventricular tachycardia. Since sinus conducted QRS complexes cannot co-exist together with ventricular tachycardia, this must all be artifact. The rhythm terminated before it could be captured on 12-lead. Upon questioning, the patient reported palpitations.
I sent it to 2 of my ECG nerd colleagues with no clinical information whatsoever, who instantly said: "Looks like afib with subendocardial ischemia and right heart strain pattern." "I Tachycardia is of course, quite common in patients following cardiac arrest. The rhythm is rapid AFib. ECG #2 shows restoration of sinus rhythm.
We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW.
See this even more interesting and more dramatic and fascinating case: History of Hypertrophic Cardiomyopathy (HOCM), with Tachycardia and High Lactate = My Comment by K EN G RAUER, MD ( 10/28 /2023 ): = QUESTION: For clarity in Figure-1 — I've reproduced today's ECG without the long lead rhythm strip. Abnormal ST-T wave abnormalities.
Answer : you must treat the patient's underlying condition causing sinus tachycardia, and repeat the ECG at the lower heart rate. They measured QTc while patients were in Afib and then again after conversion, when they were in sinus rhythm. I (Smith) measure the QT at 320 ms The Bazett-corrected QTc is divided by square root of 0.36
TiCM is defined as the presence of a reversible form of LV dysfunction due solely to an increase in ventricular rate from any type of frequent or sustained tachycardia ( rapid AFib being the most common precipitating rhythm but TiCM has also been shown to arise from AFlutter, reentry SVT rhythms, ATach, frequent PVCs, episodes of VT ).
Figure-1: While at first glance the rhythm in Figure-1 might be mistaken for sinus tachycardia in fact, this is not the rhythm. If the upright deflection in lead V1 was a single sinus P wave then the PR interval would be longer-than-expected for this to be sinus tachycardia. Figure-1: The initial ECG in today's case.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content