This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Casting doubt on value based cardiac care, a JAMA study found that outpatient cardiology practices enrolled in an accountable care organization (ACO) through the Medicare Shared Savings Program (MSSP) dont offer better care than non-ACO practices. No changes in CVD drug prescriptions, LDL profiles, or smoking cessation.
At the time, it seemed that virtually all cardiac patients with chronic AFib or heart failure were on this medication. IV Digoxin may begin to slow the ventricular response of AFib or AFlutter sooner than many clinicians realize. Smith — the choice of IV Digoxin was appropriate and effective in today's case.
Electrical cardioversion may be recommended for you if you have certain types of arrhythmias, such as: Atrial fibrillation (AFib): This is the most common type of arrhythmia, and it can cause symptoms like dizziness, fatigue, and difficulty breathing. Atrial flutter: This is a rapid but regular heart rhythm often progressing to AFib.
Case sent by Magnus Nossen MD, edits by Meyers A previously healthy woman in her 60s presented to an outpatient clinic for palpitations. Patient was referred to electrophysiologic testing due to suspicion of afib and WPW. During electrophysiologic testing AVRT was induced, which degenerated to afib with ortho and antidromic conduction.
Hopefully a repeat echocardiogram will be performed outpatient. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). Systolic function normal by visual assessment only, unable to visualize well for further characterization. 1900: RBBB and LAFB are almost fully resolved.
I sent it to 2 of my ECG nerd colleagues with no clinical information whatsoever, who instantly said: "Looks like afib with subendocardial ischemia and right heart strain pattern." "I The rhythm is rapid AFib. As noted above — it is not uncommon to see transient ST elevation with rapid AFib that resolves once the rate slows.
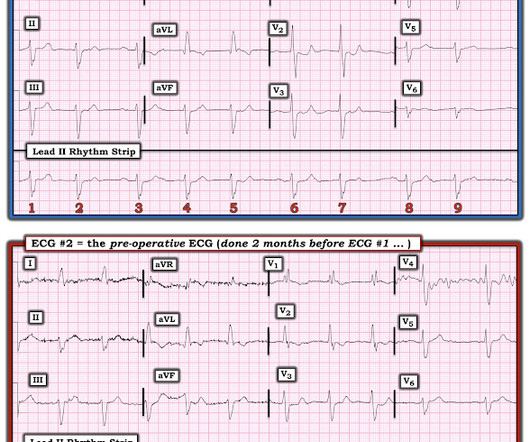
If the patient does not present with syncope, then outpatient management is probably OK, with referral to cardiology. That said — I strongly suspect that instead of AFib — that this patient was in the same 2nd-Degree, Mobitz I AV Block on the pre-operative ECG , that was done 2 months earlier ( = ECG #2 in Figure-4 ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content