

Arrhythmia? Ischemia? Both? Electricity, drugs, lytics, cath lab? You decide.
Dr. Smith's ECG Blog
NOVEMBER 26, 2018
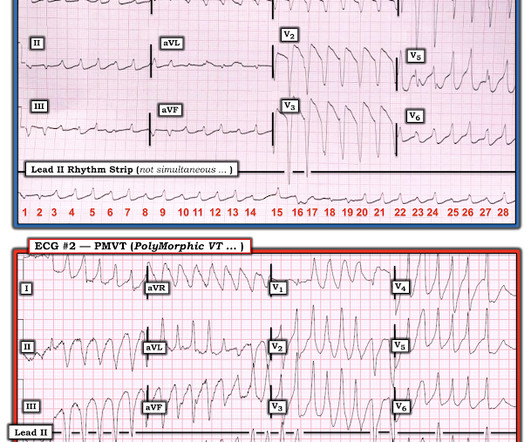
In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished. 2) Tachycardia to this degree can cause ST segment changes in several ways. Again, not an expected outcome with diltiazem).
















Let's personalize your content