This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Patients undergoing atrial fibrillation (AFib) ablation who were not properly anticoagulated and did not undergo preprocedural transesophageal echocardiogram (TEE) were significantly more likely to suffer from transient ischemic attack (TIA) or pulmonary embolism (PE).
In the pre-hospital setting the varying modalities needed to rule-in/rule-out these causative factors are not available (eg, Chest X-ray, Echocardiogram, etc). And since common things are common, the statistical probability favors Atrial Fibrillation (AFib) as the culprit. AFib can come and go. AFib can come and go.
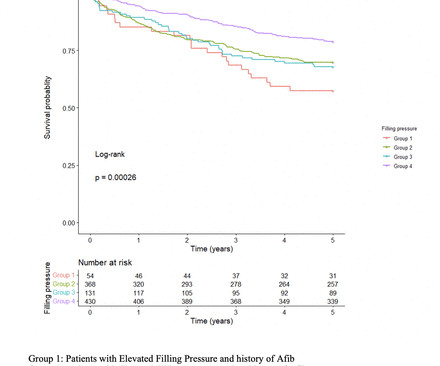
However, the impact of elevated FP as detected by pretranscatheter aortic valve replacement (TAVR) echocardiogram on long-term outcomes after TAVR remains unclear. The presence of elevated FP was determined in accordance with the latest guidelines using the last available comprehensive echocardiogram prior to TAVR.
Preprocedural transesophageal echocardiogram (TEE) has been a routine component of atrial fibrillation (AF) ablation procedures since the origin of this procedure. However, practice changes regarding preprocedural imaging and anticoagulation management have reduced the necessity of pre-ablation TEE.
That said — distinction between "classic" HCM vs the apical HCM for m may be useful because: i ) ECG findings tend to be different ( Lyon et al — Europace 20:102-112iii, 2018 ) ; — ii ) Echo appearance is different when hypertrophy localizes to the apex; and , iii ) There is a significantly greater incidence of AFib with apical HCM.
She was known to have a history of poorly controlled COPD, AFib, and multivessel coronary disease. Echocardiogram showed LVEF 55%, indeterminate diastole (due to AFib), and no significant valve pathology. David Didlake, FF/EMT-P, AG-ACNP @DidlakeDW An elder female presented to the ED with worsening shortness of breath.
Hopefully a repeat echocardiogram will be performed outpatient. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). Systolic function normal by visual assessment only, unable to visualize well for further characterization. 1900: RBBB and LAFB are almost fully resolved.
See this case: what do you think the echocardiogram shows in this case? With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common.
An echocardiogram was done. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). Is there also Brugada? Here is the result: The estimated left ventricular ejection fraction is 50 %. There is no left ventricular wall motion abnormality identified. Right ventricular prominence.
The Low EF AI will be added to Eko’s SENSORA Cardiac Early Detection Platform , the latest advancement to the platform which already features FDA-cleared algorithms to identify AFib and structural heart murmurs, often an indicator of valvular heart disease. for detection of LVEF below 40%, 84.8% sensitivity, and 69.5%
AFib Facts and Impacts Atrial fibrillation is the most common cardiac arrhythmia, affecting 2% of individuals worldwide. Before the procedure, patients should have an electrocardiogram (ECG) and echocardiogram (ultrasound of the heart) to check the heart’s rhythm and function.
Conditions such as AFib are often said to be associated with stroke as a consequence of cardioembolism. Another way of imaging the heart is via a transesophageal echocardiogram. Keywords: Cryptogenic strokes; AF; Afib; PFO; stroke; blood clots; thrombophilia; Antiphospholipid syndrome. This is called cardioembolism.
While awaiting transfer to the cath lab, STAT echocardiogram was performed and showed LVEF 30-35%, as well as anterior, inferior, and apical hypokinesis, and apical thrombus. The April 6, 2023 post — excessive baseline artifact misdiagnosed as AFib ( instead of sinus rhythm with AV Wenckebach — as in Figure-4 in this post ).
Later, he underwent a formal echocardiogram: Very severe left ventricular enlargement (LVED diameter 7.4 A bedside POC cardiac ultrasound was done: Findings: Decreased left ventricular systolic function. The patient was given furosemide and admitted to the hospital. No left ventricular wall motion abnormality identified.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content