This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I went to the patient's chart: Elderly woman with stuttering chestpain and SOB, and dizziness. Tall R wave in lead V1 and/or early transition in the chest leads ( reflecting increased "septal" forces ). WPW Cardiac arrhythmias ( including AFib ). What do you think now? Abnormal ST-T wave abnormalities.
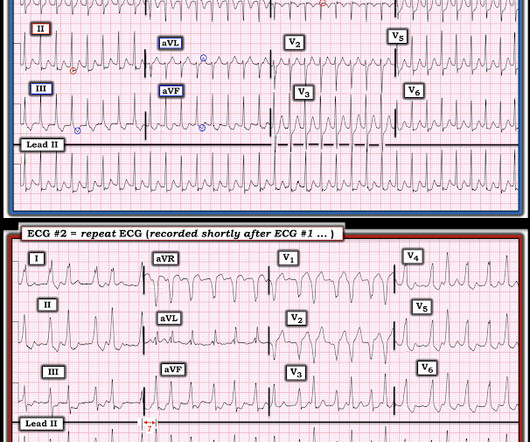
A 30-something presented with chestpain, palpitations, and SOB. Since the ventricular response in ECG #2 is comparable to the rate range for any patient who develops new-onset AFib — definitive diagnosis of WPW was not made in today's case until the 3rd ECG was obtained. It is possible to have more than a single AP!
This does NOT seem irregularly irregular enough for AFib … Instead — there is almost “group beating” with “Wenckebach periodicity”. The QRS is VERY wide — and the very wide Q in lead I ( showing marked axis deviation ) certainly suggest a ventricular etiology.
milla1cf Thu, 01/18/2024 - 14:21 January 18, 2024 — Abbott announced the first global procedures have been conducted using the company's new Volt Pulsed Field Ablation (PFA) System to treat patients battling common abnormal heart rhythms such as atrial fibrillation (AFib). chief medical officer of Abbott's electrophysiology business.
An 80-something woman who presented with chestpain and dyspnea. That said — QOH is already highly sophisticated and accurate in her assessment of ECGs from acute chestpain patients, in which the ECG is not complicated by uncommon OMI mimics. This was texted to me. What do you think? Is this posterior OMI?
The patient has acute chestpain. Tall R wave in lead V1 and/or early transition in the chest leads ( reflecting increased "septal" forces ). WPW Cardiac arrhythmias ( especially AFib ). This was texted to me in real time. What do you think? Here was my answer: "Not ischemia. Maybe HOCM or another form of LVH.
Sent by anonymous, written by Pendell Meyers Case 1: A man in his 50s presented with acute chestpain. Click here to sign up for Queen of Hearts Access Case 2: A woman in her 60s presented with acute chestpain. Normal vital signs. Here is his ECG at triage: What do you think? Normal vitals. What do you think?
The presenting complaint was chestpain — and the patient collapsed soon after arrival in the ED. These findings suggest that instead of VT — the rhythm in Figure-1 is AFib with a fairly rapid ventricular response. Since the rhythm is supraventricular (ie, AFib ) — we can accurately assess QRS morphology.
A 50 something male was seen in the emergency room due to typical chestpain. The pain had started the same day about two hours prior to medical contact. The medical care providers ascribed the patient's chestpain to new onset atrial fibrillation with rapid ventricular response after having viewed the ECG.
Getty Images milla1cf Fri, 12/08/2023 - 08:17 December 8, 2023 — The American College of Cardiology (ACC) and the American Heart Association (AHA), along with several other leading medical associations, have issued a new guideline for preventing and optimally managing atrial fibrillation (AFib).
She did notice something slightly wrong subjectively, but had no palpitations, chestpain, or SOB, or any other symptom. I focus my comment on a few additional aspects regarding new AFib. The Importance of History: We are told that today’s patient is an otherwise healthy woman — who presented to the ED for new AFib.
Diagnosis : Atrial flutter with 1:1 conduction, with fast AV conduction made possible by sympathetic drive of exercise On arrival, we obtained another 12-lead: Unremarkable Further history: One month history of shortness of breath on exertion, denies palpitations, chestpain, orthopnea, leg swelling.
On the other hand — the ST elevation seen in lead V1 is perfectly consistent with LVH and LV "strain" ( ie, The shape of this ST-T wave in lead V1, in association with the deep S wave in this lead — is a mirror-image opposite picture of the typical expected appearance of LVH with "strain" in a lateral chest lead ).
I see the following: Although there is no long lead rhythm strip — we can see that the rhythm is AFib with a controlled ventricular response ( ie, irregularly irregular rhythm without P waves — and with a heart rate between ~70-110/minute ). Regarding Intervals: There is no PR interval ( since the rhythm is AFib ).
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
9 Hours of ChestPain and Deep Q-waves: Is it too late for Thrombolytics? As per Dr. Smith — this suggests that despite QRS widening, the rhythm in ECG #3 is AFib with a rapid ventricular response. FINAL PEARL #3: When AFib is fast — the rhythm may at first glance look like it is regular. LV Aneurysm?
This 60-something with h/o COPD and HFrEF (EF 25%) presented with SOB and chestpain. AFib is the irregularly irregular rhythm that is most commonly confused with MAT — and , AFib is much, much, much more common than true MAT. The patient in this case presented with dyspnea and chestpain. GET a 12-lead!
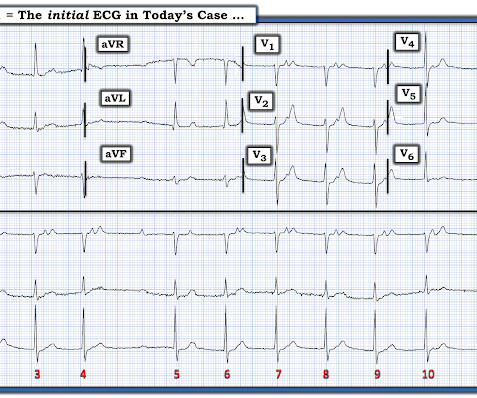
The patient also has a history of AFib and HFmrEF ( = H eart F ailure with M inimally- R educed E jection F raction ). This patient presented to the ED “after a couple of days of chest discomfort”. For clarity in Figure-1 — I have reproduced and labeled this patient’s initial ECG.
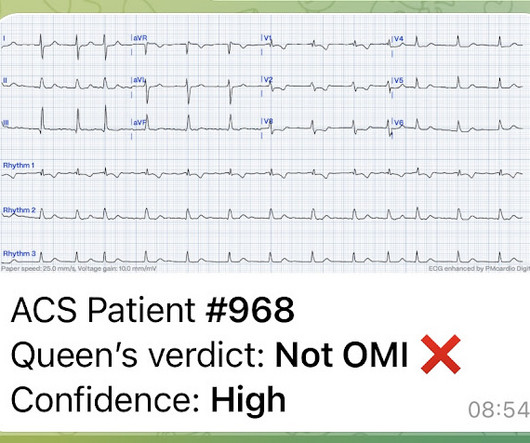
And she does not know that this is an overdose; she thinks it is a patient with chestpain!! This meets the Smith Modified Sgarbossa criteria, but the situation is wrong for diagnosing OMI!! By the way, the PM Cardio Bot Queen of Hearts says this is Not OMI with High Confidence. 3 hours later, this was recorded at a K of 2.8
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. See this case: what do you think the echocardiogram shows in this case?
and if not — Is the rhythm “irregularly irregular”, as in AFib — or is there a pattern of “regular" irregularity in the form of group beating ? ). This may lead to a series of symptoms similar to “pacemaker syndrome” ( ie, dizziness, fatigue, light-headedness, presyncope/syncope, dyspnea and/or chestpain ). What is the R ate?
There was no chestpain — and all troponins were negative. Atrial arrhythmias ( especially AFib or AFlutter ). Smith immediately knew he needed to find out what was going on with this patient! It turned out the patient had cardiac amyloidosis. The presenting complaint was cough and fever from mild Covid pneumonia.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
milla1cf Wed, 12/13/2023 - 10:24 December 13, 2023 — A new artificial intelligence (AI) model designed by Scripps Research scientists could help clinicians better screen patients for atrial fibrillation (or AFib)—an irregular, fast heartbeat that is associated with stroke and heart failure.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. Chestpain, SOB, Precordial T-wave inversions, and positive troponin. What is the Diagnosis? Now another, with ultrasound.
Written by Willy Frick A 57 year old man with was admitted to the hospital with chestpain. The April 6, 2023 post — excessive baseline artifact misdiagnosed as AFib ( instead of sinus rhythm with AV Wenckebach — as in Figure-4 in this post ). The rhythm terminated before it could be captured on 12-lead.
Here are some cases of RBBB with LAFB: What is the Diagnosis in this 70-something with ChestPain? Despite the irregularity of QRS complexes — this rhythm is not AFib — because at least some definite P waves are present ( RED arrows that I added at the bottom of ECG #1 ).
There was some dyspnea but no chestpain. Tall R wave in lead V1 and/or early transition in the chest leads ( reflecting increased "septal" forces ). WPW Cardiac arrhythmias ( especially AFib ). A young man presented with continuous prolonged generalized weakness, lightheadedness, and presyncope. Here is his ECG.
They measured QTc while patients were in Afib and then again after conversion, when they were in sinus rhythm. They found that Bazetts formula overestimated QTc in Afib while Fridericias formula was the most accurate. The RR interval was also a 10 second average. Other Research: According to this study b y Batchvarov et al. ,
This middle-aged man with no cardiac history but with significant history of methamphetamin and alcohol use presented with chestpain and SOB, worsening over days, with orthopnea. BP:143/99, Pulse 109, Temp 37.2 °C C (99 °F), Resp (!) 32, SpO2 95% On exam, he was tachypneic and had bibasilar crackles.
This patient had many complaints including chestpain. Comment by K EN G RAUER, MD ( 2/11 /2023 ): = Today’s case is from a patient with “many complaints”, including chestpain — and, an ECG that raised concern about acute anterior OMI. Chestpain was just one of these complaints. The ioninzed calcium was 6.5
1) Very high initial troponin of 45,000 ng/L 2) A full day of chestpain 3) Q-waves on the ECG, with some T-wave inversion Here is one frame of the CT scan which includes the heart: Can you spot the infarct? SUBACUTE) OMI, that would result in an undesirable delay. But this is clearly a subacute MI, with most of the damage done.
Written by Pendell Meyers A woman in her 40s presented with acute chestpain and shortness of breath. A 30-something woman with chestpain and h/o pulmonary hypertension due to chronic pulmonary emboli A 30-something with 8 hours of chestpain and an elevated troponin Syncope, Shock, AV block, Large RV, "Anterior" ST Elevation.
Sent by anonymous, written by Pendell Meyers A woman in her 40s with no known comorbidities presented with acute chestpain radiating to left arm and neck, which started approximately 4 hours prior to arrival. What is the Diagnosis in this 70-something with ChestPain? 68 minutes with chest compressions, full recovery.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content