This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Detection of Irregular Heart Rhythms Devices such as the Apple Watch or Fitbit Sense can detect irregular heart rhythms, including atrial fibrillation (AFib). These early warnings are critical, as AFib increases the risk of stroke and other heart-related complications.
Resuscitation was initiated and this ECG was obtained: Likely AFib (irregularly irregular) with bradycardia. In addition to marked bradycardia — could there be high-grade AV block? STD in V2 from posterior MI can "pull down" the STE in V1 and negate it. Figure-2: ECG #2 — recorded on arrival in the ED ( See text ).
Altered Mental Status, Bradycardia == MY Comment , by K EN G RAUER, MD ( 2/2 /2024 ): == Dr. Meyers began today’s case with the clinical challenge of asking you to identify the underlying cause of ECG #2. -- Read this ECG -- Osborn Waves and Hypothermia (this is the "Figure" above) What does LBBB look like in severe hypothermia?
Her vital signs were within normal limits except for bradycardia at 55 bpm. It is probably sinus bradycardia with very small/depressed P-waves and prolonged PR interval. P EARL # 4 In my opinion, it is not worth wasting time trying to figure out the specific rhythm diagnosis of a bradycardia when there is hyperkalemia.
during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. Thus, there is sinus bradycardia and arrhythmia sinus pauses ( which may be longlasting, ultimately leading to sinus arrest ) and SA nodal block. New slow AFib reflects a combination of these rhythm problems. second in duration.
Of 59 participants who sent at least 1 EKG, 52 (88.1%) were in sinus rhythm, 3 (5.1%) AF, 2 (3.4%) indeterminate, and 2 (3.4%) sinus bradycardia. Of 76 participants assessed by the study team, 32 (42.1%) reported anxiety surrounding notifications. Cardiac monitor demonstrated AF in 2 of 3 participants with AF on Apple Watch EKGs.
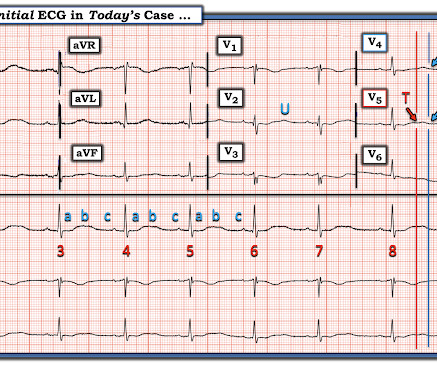
This ECG shows sinus bradycardia with massively long QT (or QU?) Especially when present in the setting of bradycardia and syncopal episodes, this is very worrisome for high risk of lethal dysrhythmias including polymorphic ventricular fibrillation (termed Torsades when in the setting of long QT). interval, at over 600 msec.
Sinus bradycardia – sinus rhythm below 60 bpm is a sinus bradycardia. AFIB/AFL – atrial fibrillation or atrial flutter episodes. Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia. In healthy individuals occurs during exercising or strong emotions. Usually does not exceed 160 bpm.
. = My Comment by K EN G RAUER, MD ( 3/15 /2023 ): = I found today’s case highly instructive in highlighting a number of important aspects regarding the presentation and initial treatment of a patient who presents to the ED with new AFib. I focus my comment on a few additional aspects regarding new AFib.
There are 3 etiologies I always think of with bradycardia and AV block: 1. C linical P oints R egarding E CG # 1 : We are told that the patient is a middle-aged woman and that she previously had been in AFib with LBBB. She could even have developed asystole. Hyperkalemia. Her K was normal 3. Ischemia. seconds in duration.
Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). RBBB in blunt chest trauma seems to be indicative of several RV injury. Atrial fibrillation is also a predictor of worse outcomes in this case (Alborzi). Sinus Tachycardia ( common in any trauma patient. ).
Additionally, her beta-blocker dose had been decreased because of bradycardia, further predisposing her to atrial flutter. For example: Statistical likelihood that the regular WCT in ECG #1 might be AFlutter ( instead of VT ) is greatly increased in a patient with AFib who is taking Flecainide.
Similar-looking wide beats #7,13,14 must also be aberrantly conducted supraventricular impulses — and since P waves are lost after beat #6 and subsequent R-R intervals are irregular — beats #7-thru-16 constitute a run of rapid AFib.
Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. WPW Cardiac arrhythmias ( especially AFib ). Smith's — in that despite the alarming ST-T wave changes, I did not think ECG #1 was the result of an acute event. Abnormal ST-T wave abnormalities.
ie, See My Comment in the April 6, 2023 post in Dr. Smith's ECG Blog — in which AFib and AV Wenckebach were repeatedly misinterpreted by a number of medical providers over a period of months, with obvious implications regarding optimal treatment decision-making ). Laddergram Illustration: The mechanism of AV block in ECG #2 is complex.
Although unfortunately there is no long lead II rhythm strip — RED arrows in ECG #2 highlight that sinus P waves ( the rhythm is sinus bradycardia and arrhythmia ) continue throughout the tracing , allowing us to establish with certainty the 7 sinus-conducted beats vs the 2 PVCs in this tracing. Only AFib was induced during EP study.
Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). Sinus Tachycardia ( common in any trauma patient. ). RBBB ( as by far the most common conduction defect — owing to the more vulnerable anatomic location of the RV ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content