This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
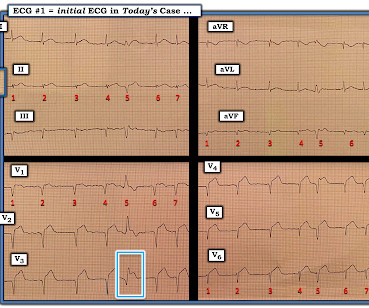
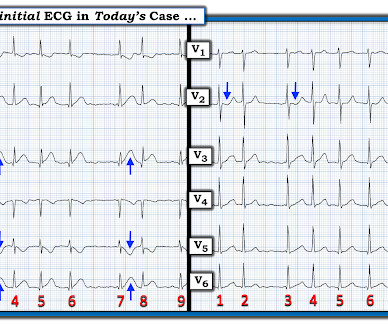
This defines the rhythm as AFib ( A trial F ibrillation ) , here with a controlled ventricular response ( ie, overall heart rate between ~70-to-100/minute ). IMPRESSION: In this patient who presents with severe, new-onset CP — today's ECG is diagnostic of an extensive, ongoing antero-lateral STEMI. Smith's ECG Blog ). =
These findings suggest that instead of VT — the rhythm in Figure-1 is AFib with a fairly rapid ventricular response. Since the rhythm is supraventricular (ie, AFib ) — we can accurately assess QRS morphology. Given a lack of prior history — I don’t know if the AFib on ECG #1 is ( or is not ) a new finding.
I see the following: Although there is no long lead rhythm strip — we can see that the rhythm is AFib with a controlled ventricular response ( ie, irregularly irregular rhythm without P waves — and with a heart rate between ~70-110/minute ). Regarding Intervals: There is no PR interval ( since the rhythm is AFib ).
ECG Blog #185 — Review of the P s, Q s, 3 R Approach for systematic rhythm interpretation. ECG Blog #271 — Reviews the concept of diffuse Subendocardial Ischemia. ECG Blog #316 — The patient died. ECG Blog #184 — That magical inverse relationship between leads III and aVL. ECG Blog #183 — deWinter-like T waves.
In this ECG Cases blog Dr. Jesse McLaren guides us through 10 cases, driving home the points that sepsis is a common cause of rapid Afib and diffuse ST depression with reciprocal ST elevation in aVR, myo/pericarditis is a diagnosis of exclusion, endocarditis or lyme carditis can cause AV block, PE can cause low grade fever and ECG signs of acute RV (..)
Another missed OMI by the False STEMI-NonSTEMI Dichotomy Don't miss them!!! We are not told IF this AFib is new ( as a result of the acute LAD OMI ) — or, if this AFib is this patient's longstanding rhythm ( nor are we told if the patient is on anticoagulation or is taking rate-slowing medication ).
This is written by Magnus Nossen, with some edits by Smith This ECG diagnosis will be obvious to the majority of the readers of this blog. Notice that much of the dark blue is concentrated on the QRS (R-wave); the QRS is totally ignored in the STEMI paradigm!! It is not obvious for the majority of doctors or even cardiologists.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
There is STE in III and aVF which does not meet STEMI criteria due to insufficient STE in lead aVF. Resuscitation was initiated and this ECG was obtained: Likely AFib (irregularly irregular) with bradycardia. The cardiologists were not familiar with this and insisted that the ECG in paced rhythm could not be used to "look for a STEMI".
I sent it to 2 of my ECG nerd colleagues with no clinical information whatsoever, who instantly said: "Looks like afib with subendocardial ischemia and right heart strain pattern." "I The rhythm is rapid AFib. As noted above — it is not uncommon to see transient ST elevation with rapid AFib that resolves once the rate slows.
Dyspnea, Right Bundle Branch block, and ST elevation Here are two more cases where the differential diagnosis is acute OMI vs. LV aneurysm: Is this acute STEMI? As per Dr. Smith — this suggests that despite QRS widening, the rhythm in ECG #3 is AFib with a rapid ventricular response. LV Aneurysm? Would you give Thrombolytics?
Any objective, rule-based analysis of this ECG would scream "STEMI" or "OMI". And I recognized this as a STEMI mimic. WPW Cardiac arrhythmias ( especially AFib ). There are Q-waves in V4-V6, with what appear to be hyperacute T-waves. But, alas, ECGs are like faces. No measurements can tell you the identity of the face.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. Is that an obvious STEMI underneath that rhythm? Is this inferor STEMI? Atrial Flutter with Inferior STEMI? If I fix the rhythm will the ST changes resolve?
The computer called this Acute STEMI What do you think? STEMI never has a very short QT. There is Bazett, Fridericia, Hodges, Framingham and Rautaharju -- see here at mdcalc: [link] If the ST Elevation here were due to STEMI, it would be an LAD Occlusion. is: i ) SQTS ( S hort QT S yndrome ) ; and , ii ) Hypercalcemia.
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. There are new Q-waves in aVL, V5-6. The March 17, 2023 post — for PTA.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content