This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
For more regarding ECG criteria for LVH — See the ADDENDUM below and/or ECG Blog #73 and ECG Blog #245. My written interpretation on a tracing such as this one would read, "Marked LVH and 'strain' and/or ischemia — with need for clinical correlation." WPW Cardiac arrhythmias ( including AFib ).
M Y T houghts on the ECG in Figure-1: I have presented similar ECGs to the one in today's tracing on several occasions ( most recently in ECG Blog #284 ). M y I MPRESSION : The rhythm in Figure -1 is almost certain to be very rapid AFib in a patient with WPW. The patient was hemodynamically stable in association with this rhythm. (
This ST depression appears to be maximal in leads V3-to-V5 — which could reflect acute posterior OMI ( O cclusion-based M yocardial I nfarction ) — most probably with multi -vessel disease ( ie, diffuse subendocardial ischemia suggested by the ST depression with ST elevation in aVR>V1 ). ECG Blog #316 — The patient died.
These findings suggest that instead of VT — the rhythm in Figure-1 is AFib with a fairly rapid ventricular response. Since the rhythm is supraventricular (ie, AFib ) — we can accurately assess QRS morphology. Shark Fin" ST segment elevation is most often a sign of severe transmural ischemia that results from acute coronary occlusion.
I see the following: Although there is no long lead rhythm strip — we can see that the rhythm is AFib with a controlled ventricular response ( ie, irregularly irregular rhythm without P waves — and with a heart rate between ~70-110/minute ). Regarding Intervals: There is no PR interval ( since the rhythm is AFib ).
See our other blog posts of hypothermia and Osborn waves -- Massive Osborn Waves of Severe Hypothermia (23.6 The rhythm is irregularly irregular, and appears to be AFib with a fairly slow ventricular response ( overall rate <70/minute ) — although marked baseline artifact renders the search for atrial activity futile.
In addition — there is transmural ischemia of the septum , most often resulting from occlusion proximal to the 1st septal perforator branch of the LAD. The rhythm in both tracings in Case #2 shows AFib with a controlled ventricular response ( with a PVC in the 2nd tracing ).
In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished. First , there can simply be diffuse ST depressions (which obligates reciprocal STE in aVR) associated with tachycardia which are not indicative of ischemia.
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). There is STE in aVR. Thus, there is high lateral OMI with diffuse ST depression. Moreover, left main occlusion often presents near death.
The unique " shape " of the prominent ST-T wave abnormalities in this tracing — that are much more suggestive of some significant form of LVH ( L eft V entricular H ypertophy ) rather than ischemia. For more on Giant T waves — See My Comment at the bottom of the page in the June 22, 2020 and September 19, 2022 posts in Dr. Smith's ECG Blog ).
My Comment , by K EN G RAUER, MD ( 7/5/2018 ): This blog post provides an excellent example of how a patient with SSS ( = S ick S inus S yndrome ) may present. Many patients have a T achy- B rady syndrome in which tachyarrhythmias ( most commonly rapid AFib ) alternate with periods of bradycardia. second in duration.
. = My Comment by K EN G RAUER, MD ( 3/15 /2023 ): = I found today’s case highly instructive in highlighting a number of important aspects regarding the presentation and initial treatment of a patient who presents to the ED with new AFib. I focus my comment on a few additional aspects regarding new AFib.
ACUTE MI (I allowed Acute MI to be in the report because I knew there would be an elevated troponin from ischemia, which is the definition of acute MI -- but in this case it would most likely be a Type 2 MI from tachycardia) There is also LA-RA lead reversal. The rhythm is rapid AFib. Atrial fib may cause Occlusion mimic."
There was no evidence of ischemia. C linical P oints R egarding E CG # 1 : We are told that the patient is a middle-aged woman and that she previously had been in AFib with LBBB. While I agree that AFib + complete AV block is the most likely rhythm diagnosis I'd like to see additional monitoring strips to be sure.
This is written by Magnus Nossen, with some edits by Smith This ECG diagnosis will be obvious to the majority of the readers of this blog. Thoughts about Today's CASE: On occasion — a patient may present for acute care because of CP ( C hest P ain ) due solely to a tachyarrhythmia ( including new AFib, a reentry SVT or VT ).
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. The rhythm is atrial fibrillation. The QRS complex is within normal limits. These include.
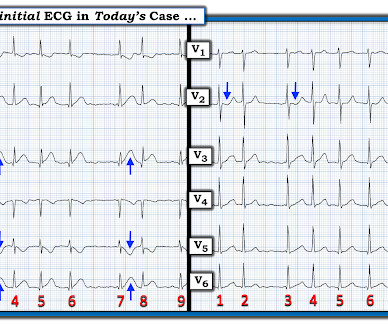
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. I've copied KEY points from My Comment in the August 6, 2022 post in Dr. Smith's ECG Blog — regarding the answer to this question. Chest trauma was suspected on initial exam. Figure-1: The initial ECG in today's case.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
Here is her post-cardioversion ECG: ECG#2 - Immediately post cardioversion: Appropriate ST depression maximal in V5-6 and lead II, secondary to subendocardial ischemia, likely residual from the preceding tachycardia. Patient was referred to electrophysiologic testing due to suspicion of afib and WPW. She was sedated and cardioverted.
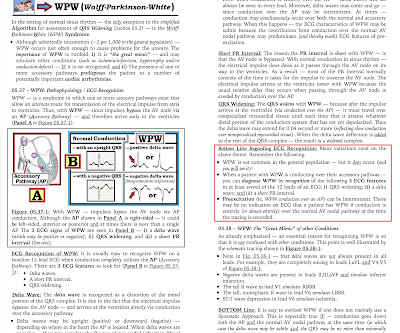
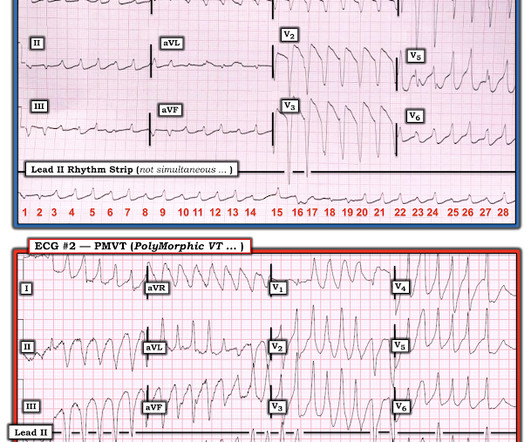
MY THOUGHTS on ECG #1: My initial impression on looking at the ECG in Figure-1 — was that the rhythm was either rapid AFib in a patient with WPW — or — PMVT ( P oly M orphic VT ). The reason I initially thought the underlying rhythm was AFib — is that no atrial activity is seen in any lead and the rhythm “looks” irregular. See text ).
The QRS is wide in B — but the rhythm is irregularly irregular with no sinus P waves — so this most probably represents rapid AFib with an atypical RBBB/LPHB morphology. We now see that QRS morphology in lead II during sinus rhythm is similar to the QRS morphology in lead II during rapid AFib (beats #1-5 in lead II in A).
Is This a Simple Right Bundle Branch Block? == MY Comment , by K EN G RAUER, MD ( 1/26/2020 ): == Dr. Smiths ECG Blog has presented too-numerous-to-count cases of hyperkalemia ( See My Comment in the 12/11/2018 post there are many others! ). Is this just right bundle branch block?
As we've discussed on numerous other posts in Dr. Smith's ECG Blog ( See My Comment at the bottom of the page in the May 5, 2022 post) — a growing number of conditions other than Brugada Syndrome have been found to temporarily produce a Brugada-1 ECG pattern. What are the ECG Findings of Cardiac Contusion?
Here was my answer: "Not ischemia. WPW Cardiac arrhythmias ( especially AFib ). This was texted to me in real time. The patient has acute chest pain. What do you think? Maybe HOCM or another form of LVH. I would not activate cath lab. Abnormal ST-T wave abnormalities. Conduction defects (ie, LBBB, IVCD ).
There is no evidence of infarction or ischemia. I focus My Comment on determination of the e tiology of this patient’s tachyarrhythmia — and compare it to other SVT rhythms previously published in Dr. Smith’s ECG Blog. E CG # 2 in Figure-1 is from the October 16, 2019 post on Dr. Smith’s Blog. H eart R ate C an H elp !
Meyers' discussion — he lists more than 20 links to cases that we've presented related to this entity on Dr. Smith's ECG Blog. That said — the diagnosis of acute PE continues to be overlooked ( and the ECGs of such patients continue to be misinterpreted as acute ischemia or infarction — instead of being recognized as diagnostic of acute PE ).
Compared to TTE from 7/3/24: the anterior regional wall motion abnormality is new and is consistent with ischemia/infarction in the LAD territory == MY Comment , by K EN G RAUER, MD ( 11/20 /2024 ): == There are several insightful aspects of today's case. Regional wall motion abnormality--mid anterior akinesis.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content