This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
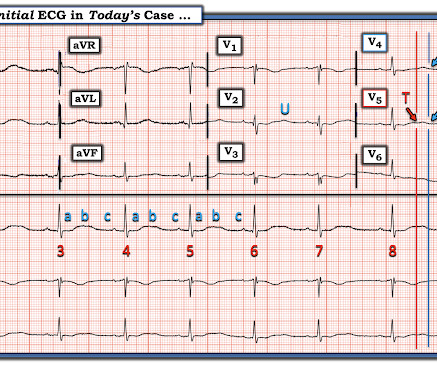
Especially when present in the setting of bradycardia and syncopal episodes, this is very worrisome for high risk of lethal dysrhythmias including polymorphic ventricular fibrillation (termed Torsades when in the setting of long QT). This ECG shows sinus bradycardia with massively long QT (or QU?) interval, at over 600 msec.
See these publications for more information Overall, management for cardiac contusion is mostly supportive unless surgical complications develop, involving appropriate treatment of dysrhythmias and hemodynamic instability. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ).
I sent it to 2 of my ECG nerd colleagues with no clinical information whatsoever, who instantly said: "Looks like afib with subendocardial ischemia and right heart strain pattern." "I The rhythm is rapid AFib. As noted above — it is not uncommon to see transient ST elevation with rapid AFib that resolves once the rate slows.
Atrial dysrhythmias, and atrial fi brillation in particular, are frequently misdiagnosed by computer algorithms and then by the physician who overreads them. M Y A NSWER: The issue of whether C omputerized E CG I nterpretations are “at fault” for an inaccurate ECG diagnosis has been addressed numerous times on this blog. GET a 12-lead!
Here is one full text article on the topic from Clinical Cardiology 2008: Diagnostic Approach and Treatment Strategy in Tachycardia-induced Cardiomyopathy Atrial Tachycardia (AT): another SVT in the ED Rapid dysrhythmia from non-sinus focus above AV node. E CG # 2 in Figure-1 is from the October 16, 2019 post on Dr. Smith’s Blog.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content