This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Blood was drawn , and the patient was promptly placed in a room to be seen — but on entering, the ED physician found her unresponsive in cardiacarrest. Do you see any indication on this ECG of WHY this patient was about to arrest? Is there any indication on this ECG of WHY this patient shortly after had a cardiacarrest?
While on telemetry monitoring he suffered cardiacarrest and was resuscitated. What ECG finding may have contributed to (or precipitated) the cardiacarrest? Learning points : Takotsubo can lead to cardiacarrest from ventricular arrhythmia. There are no clear signs of OMI. There is a prolonged QTc.
See our other blog posts of hypothermia and Osborn waves -- Massive Osborn Waves of Severe Hypothermia (23.6 C), with Cardiac Echo -- A Pathognomonic ECG. His temperature was brought back to normal over time in the ICU. He was extubated and had normal neurologic function. He did well and was discharged.
At some point ~1-2 hours after the initial ECG — the patient developed runs of VT, leading to cardiacarrest. ECG Blog #185 — Review of the P s, Q s, 3 R Approach for systematic rhythm interpretation. ECG Blog #271 — Reviews the concept of diffuse Subendocardial Ischemia. ECG Blog #316 — The patient died.
NOTE: The ECGs in today's case are recorded in the Cabrera Format ( See Dr. Grauer Comment in the October 26, 2020 post of Dr. Smith's ECG Blog for review on the Cabrera Format ). KEY Point: Nothing other than AFib with WPW results in a ventricular response this fast ( which is why Figure-2 is pathognomonic for AFib in a patient with WPW ).
I sent it to 2 of my ECG nerd colleagues with no clinical information whatsoever, who instantly said: "Looks like afib with subendocardial ischemia and right heart strain pattern." "I He had multiple cardiacarrests with ROSC regained each time. This patient arrested shortly after hospital arrival.
Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiacarrest, cardiogenic shock or impending shock. Suffice it to say that, "The heart does whatever it will do when a patient is about to arrest". RBBB + LAFB in the setting of ACS is very bad.
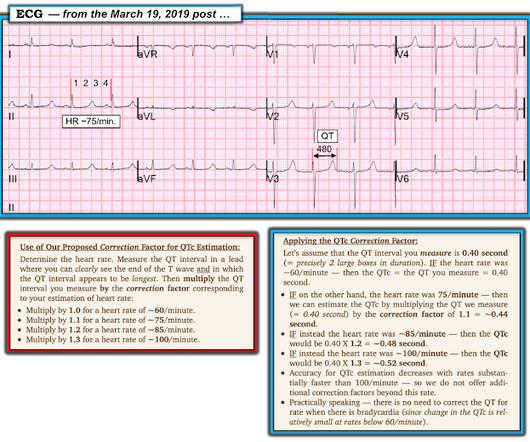
Figure-2: A rapid method for estimating the QTc ( Figure from My Comment in the March 19, 2019 post in Dr. Smith's ECG Blog ). == Clinical Implications of a Short QTc: The differential diagnosis for today's tracing, with its short QTc ~360 msec. ) — but as can be seen, my estimate of ~360 msec.
This was a very complex case and the details are too much for an ECG Blog, but suffice it to say that, s hortly thereafter, the patient had an asystolic arrest and was resuscitated. He was placed on ECMO. Peak troponin I at 24 hours was 480 ng/L. Laddergram Illustration: The mechanism of AV block in ECG #2 is complex.
With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Thirty-six patients (36%) presented with cardiacarrest, and 78% (28/36) underwent emergent angiography. See this case: what do you think the echocardiogram shows in this case? A normal PR interval.
As we've discussed on numerous other posts in Dr. Smith's ECG Blog ( See My Comment at the bottom of the page in the May 5, 2022 post) — a growing number of conditions other than Brugada Syndrome have been found to temporarily produce a Brugada-1 ECG pattern. What are the ECG Findings of Cardiac Contusion?
See these other related cases: A patient with cardiacarrest, ROSC, and right bundle branch block (RBBB). Rather than AFib I suspect we are seeing a sinoventricular rhythm in ECG #1 with some sinus arrhythmia. Is this just right bundle branch block? large boxes, but then decreases and remains slightly irregular ).
Features of Short QT Syndrome: From My Comment at the bottom of the page in the September 2, 2019 post of Dr. Smith’s ECG Blog: SQTS is an inherited cardiac channelopathy determined by the presence of symptoms ( syncope, cardiacarrest ) — positive family history — and the ECG finding of an abnormally short QTc interval.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content