This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Given the irregular irregularity of beats #4-through 17 — Is this a run of AFib ( A trial Fib rillation ) with aberrant conduction? This raises the question if beats #4-thru-17 might represent a run of AFib with aberrant conduction? For more on fusion beats — See ECG Blog #128 and Blog #129 ). See ECG Blog #133 ).
PEARL # 2: When the rate of AFib is rapid — this irregular tachycardia may look regular when it is not. That the rhythm is AFib — is easier to appreciate in Figure-3. Clearly, the rhythm is AFib — here with a controlled ventricular response. ECG Blog #240 — reviews my approach to the ECG assessment of regular SVT rhythms.
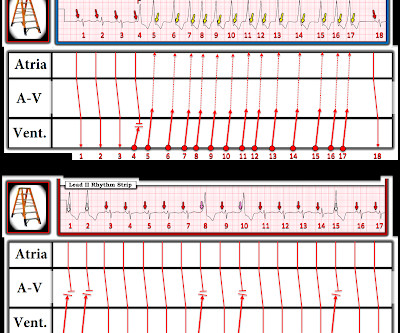
PEARL # 1: As I emphasize in ECG Blog #148 ( from where I took the tracing I show in Figure-3 ) — the BEST way to prove artifact — is to recognize persistence of an underlying spontaneous rhythm that is unaffected by any erratic or suspicious deflections that are seen. Figure-3: I've reproduced this tracing from ECG Blog #148 ( See text ). =
For more regarding ECG criteria for LVH — See the ADDENDUM below and/or ECG Blog #73 and ECG Blog #245. A bout H CM ( Different Forms of this Entity ): I've excerpted what appears below from My Comment in the December 26, 2023 post in Dr. Smith's ECG Blog. WPW Cardiac arrhythmias ( including AFib ).
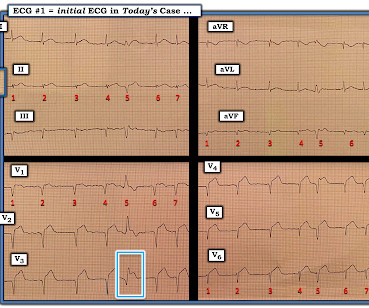
This defines the rhythm as AFib ( A trial F ibrillation ) , here with a controlled ventricular response ( ie, overall heart rate between ~70-to-100/minute ). R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. ECG Blog #230 — Reviews how to compare serial ECGs.
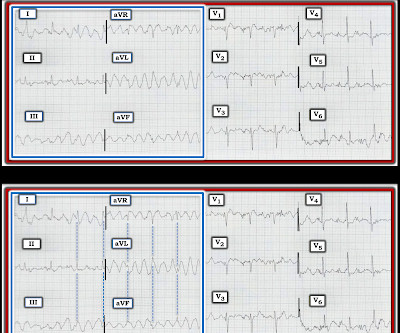
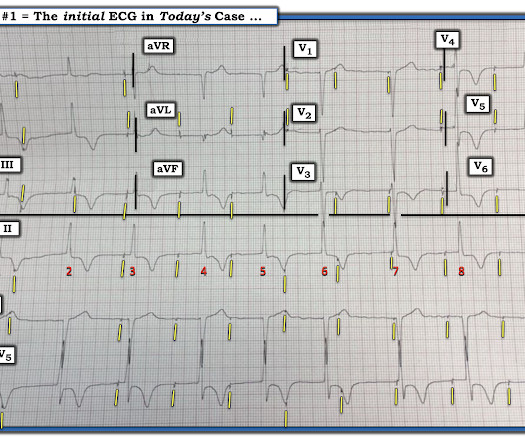
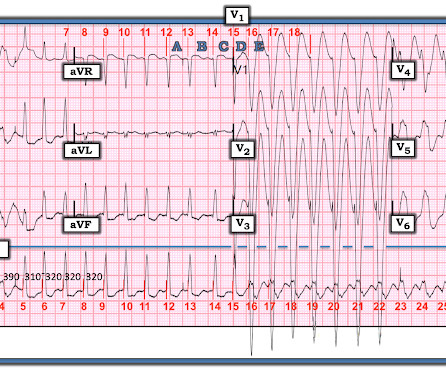
I was sent the ECG shown in Figure-1 — being told only that providers on the case suspected AFib ( A trial Fib rillation ) with RBBB ( R ight B undle B ranch B lock ) aberrancy. As reviewed in ECG Blog #231 — QRS morphology in VT may manifest a number of different forms. How certain are YOU of your answer?
NOTE: For more on ECG recognition of RVH and/or pulmonary hypertension ( re the qR pattern in lead V1 ) — See ECG Blog #234 and Blog #248. This could have been an optimal time to try a Lewis Lead — which sometimes reveals atrial activity not evident with standard lead placement ( See ECG Blog #223 ).
M Y T houghts on the ECG in Figure-1: I have presented similar ECGs to the one in today's tracing on several occasions ( most recently in ECG Blog #284 ). M y I MPRESSION : The rhythm in Figure -1 is almost certain to be very rapid AFib in a patient with WPW. The patient was hemodynamically stable in association with this rhythm. (
By the P s, Q s, 3 R Approach ( See ECG Blog #185 ): Regarding R egularity — the rhythm is irregularly irregular. As a result — IF the 1 lead you are monitoring happens to be one in which P waves are not well seen — then you might assume the irregular rhythm in front of you was AFib. ECG Blog #199 — for Review of M AT.
These findings suggest that instead of VT — the rhythm in Figure-1 is AFib with a fairly rapid ventricular response. Since the rhythm is supraventricular (ie, AFib ) — we can accurately assess QRS morphology. Given a lack of prior history — I don’t know if the AFib on ECG #1 is ( or is not ) a new finding.
I see the following: Although there is no long lead rhythm strip — we can see that the rhythm is AFib with a controlled ventricular response ( ie, irregularly irregular rhythm without P waves — and with a heart rate between ~70-110/minute ). Regarding Intervals: There is no PR interval ( since the rhythm is AFib ).
By the P s , Q s , 3 R Approach ( See ECG Blog #185 ): The rhythm in Figure-1 is clearly not R egular. PEARL #2: As cited in ECG Blog #252 — my favorite truism in arrhythmia interpretation is, "The commonest cause of a pause is a blocked PAC". ECG Blog #185 — Review of the P s, Q s, 3 R Approach for systematic rhythm interpretation.
NOTE: The ECG in Figure-1 has been recorded at the usual 25mm/second speed — but with the Cabrera format ( Please see my Editorial Note near the top of the page in ECG Blog #365 for review of the basics of this recording system ). Among the fast Supraventricular Rhythms: This is not AFib — because the rhythm is regular.
In this ECG Cases blog Dr. Jesse McLaren guides us through 10 cases, driving home the points that sepsis is a common cause of rapid Afib and diffuse ST depression with reciprocal ST elevation in aVR, myo/pericarditis is a diagnosis of exclusion, endocarditis or lyme carditis can cause AV block, PE can cause low grade fever and ECG signs of acute RV (..)
NOTE: The ECGs in today's case are recorded in the Cabrera Format ( See Dr. Grauer Comment in the October 26, 2020 post of Dr. Smith's ECG Blog for review on the Cabrera Format ). KEY Point: Nothing other than AFib with WPW results in a ventricular response this fast ( which is why Figure-2 is pathognomonic for AFib in a patient with WPW ).
See our other blog posts of hypothermia and Osborn waves -- Massive Osborn Waves of Severe Hypothermia (23.6 The rhythm is irregularly irregular, and appears to be AFib with a fairly slow ventricular response ( overall rate <70/minute ) — although marked baseline artifact renders the search for atrial activity futile.
This blog explores the ways wearable technology can help track heart health, the advantages it offers, and how it contributes to better outcomes for those requiring surgical intervention. These early warnings are critical, as AFib increases the risk of stroke and other heart-related complications.
This does NOT seem irregularly irregular enough for AFib … Instead — there is almost “group beating” with “Wenckebach periodicity”. The QRS is VERY wide — and the very wide Q in lead I ( showing marked axis deviation ) certainly suggest a ventricular etiology.
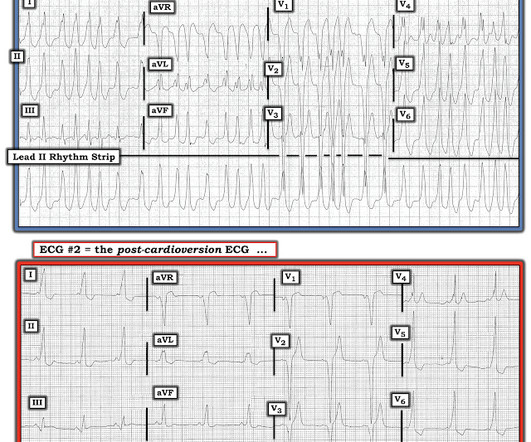
Since the ventricular response in ECG #2 is comparable to the rate range for any patient who develops new-onset AFib — definitive diagnosis of WPW was not made in today's case until the 3rd ECG was obtained. FINAL Points in Today's CASE: Even though the SPERRI value during AFib in today's case was not below 250 msec.
The rhythm in both tracings in Case #2 shows AFib with a controlled ventricular response ( with a PVC in the 2nd tracing ). Presumably the AFib is not a new rhythm — since new-onset AFib is usually associated with a rapid ventricular response.
Is longterm endurance-training a risk factor for AFib and AFlutter? == Why is Today's Initial Rhythm AFlutter? The answer to this question is fascinating — albeit extending beyond the scope of this ECG Blog. Smith immediately say the rhythm was AFlutter with 1:1 AV conduction? Does Exercise Induce Non-Sinus Tachyarrhythmias?
Jesse McLaren explains his AFIB mnemonic for approach to atrial fibrillation that involves 4 questions: 1. and runs through 10 cases to elucidate the nuances of atrial fibrillation management on this ECG Cases blog. Is it atrial fibrillation? Does the patient need an anticoagulant started in the ED?
As I discussed in detail in My Comment at the bottom of the page in the January 13, 2024 post in Dr. Smith's ECG Blog — pacemaker spikes tend to be a high frequency signal. The April 6, 2023 post — excessive baseline artifact misdiagnosed as AFib ( instead of sinus rhythm with AV Wenckebach — as in Figure-4 in this post ).
. = My Comment by K EN G RAUER, MD ( 3/15 /2023 ): = I found today’s case highly instructive in highlighting a number of important aspects regarding the presentation and initial treatment of a patient who presents to the ED with new AFib. I focus my comment on a few additional aspects regarding new AFib.
As per Dr. Meyers — the underlying rhythm is either slow AFib or a junctional escape rhythm ( There is a fairly-but- not -completely regular underlying bradycardic rhythm — with narrow QRS — and no P waves ).
My Comment , by K EN G RAUER, MD ( 7/5/2018 ): This blog post provides an excellent example of how a patient with SSS ( = S ick S inus S yndrome ) may present. Many patients have a T achy- B rady syndrome in which tachyarrhythmias ( most commonly rapid AFib ) alternate with periods of bradycardia. second in duration.
For more on Giant T waves — See My Comment at the bottom of the page in the June 22, 2020 and September 19, 2022 posts in Dr. Smith's ECG Blog ). WPW Cardiac arrhythmias ( including AFib ). Depth of the inverted T waves in leads V4 and V5 in Figure-1 attains this range. ( PEARL #1: Truly “giant” T waves are not overly common.
I don’t see evidence of retrograde atrial activity during the WCT — but usually with the “almost regular AFib rhythms” — you can when you measure pick up some slight differences — so my hunch is that the initial ECG is a REENTRY SVT rhythm, that then breaks down to AFib. Theoretically — this can occur with BOTH AVNRT and AVRT.
As we often emphasize ( See My Comment in the May 5, 2020 post of Dr. Smith's ECG Blog ) — Statistically (ie, even before we look at the ECG itself ) — at least 80% of all regular WCT rhythms without clear sign of P waves will turn out to be VT ( V entricular T achycardia ). I'd add the following thoughts to Dr. Smith's discussion.
The patient also has a history of AFib and HFmrEF ( = H eart F ailure with M inimally- R educed E jection F raction ). I have emphasized on many occasions in Dr. Smith's ECG Blog how AFlutter is by far (!) This patient presented to the ED “after a couple of days of chest discomfort”. Why was it Wrong to Think the Rhythm was AFlutter?
Therefore — the rhythm in ECG #1 is almost certain to be AFib ( A trial F ibrillation ) , seen here with a “rapid” ventricular response. Under normal conditions with AFib — the refractory period of the AV node does not allow more than 150-to-200 impulses/minute to be conducted to the ventricles.
This is written by Magnus Nossen, with some edits by Smith This ECG diagnosis will be obvious to the majority of the readers of this blog. Thoughts about Today's CASE: On occasion — a patient may present for acute care because of CP ( C hest P ain ) due solely to a tachyarrhythmia ( including new AFib, a reentry SVT or VT ).
Patient was referred to electrophysiologic testing due to suspicion of afib and WPW. During electrophysiologic testing AVRT was induced, which degenerated to afib with ortho and antidromic conduction. Despite the near regularity in places — the reasons I immediately thought of WPW with very rapid AFib were i ) As per per Drs.
C linical P oints R egarding E CG # 1 : We are told that the patient is a middle-aged woman and that she previously had been in AFib with LBBB. While I agree that AFib + complete AV block is the most likely rhythm diagnosis I'd like to see additional monitoring strips to be sure. Clinically What has happened in the interim?
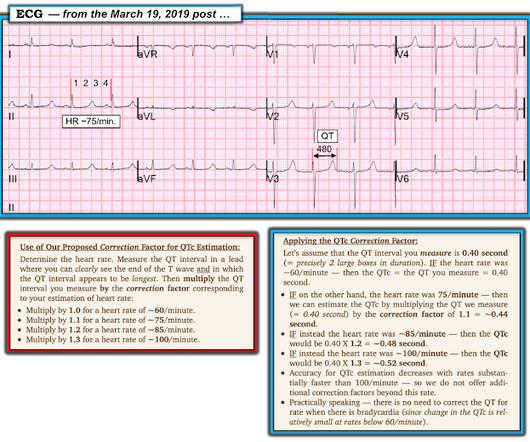
Figure-2: A rapid method for estimating the QTc ( Figure from My Comment in the March 19, 2019 post in Dr. Smith's ECG Blog ). == Clinical Implications of a Short QTc: The differential diagnosis for today's tracing, with its short QTc ~360 msec. ) — but as can be seen, my estimate of ~360 msec. mg/dL — vs normal values = 4.4-5.2
I've copied KEY points from My Comment in the August 6, 2022 post in Dr. Smith's ECG Blog — regarding the answer to this question. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). Figure-1: The initial ECG in today's case. What are the ECG Findings of Cardiac Contusion?
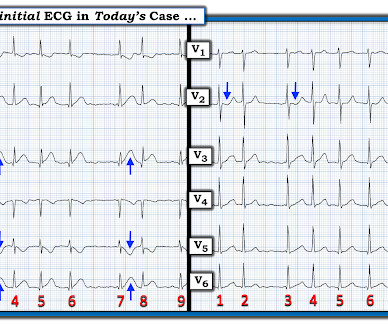
The rhythm is rapid AFib. These are the "Take-Home" Lessons from today's tracing: As per Dr. Smith — Rapid AFib may sometimes simulate acute posterior OMI. This anterior ST depression often resolves ( or at least greatly decreases ) when AFib is controlled and the heart rate slows. The QRS complex in lead I looks "funny".
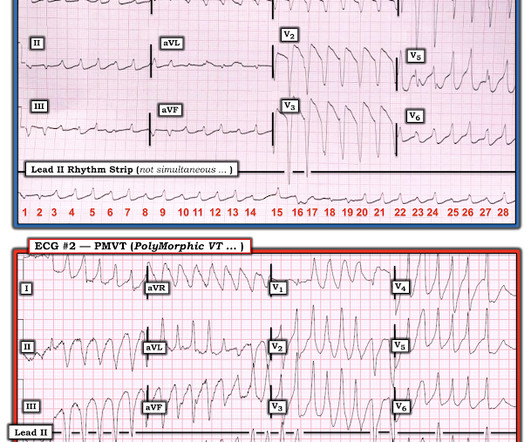
MY THOUGHTS on ECG #1: My initial impression on looking at the ECG in Figure-1 — was that the rhythm was either rapid AFib in a patient with WPW — or — PMVT ( P oly M orphic VT ). The reason I initially thought the underlying rhythm was AFib — is that no atrial activity is seen in any lead and the rhythm “looks” irregular. See text ).
This was a very complex case and the details are too much for an ECG Blog, but suffice it to say that, s hortly thereafter, the patient had an asystolic arrest and was resuscitated. He was placed on ECMO. Peak troponin I at 24 hours was 480 ng/L.
MY Thoughts on Today's ECG: As per Dr. Smith — the rhythm in ECG #1 appears to be AFib with a controlled ventricular response ( ie, irregularly irregular without clear sign of P waves ). Figure-1: The initial ECG in today's case. ( To improve visualization — I've digitized the original ECG using PMcardio ). Could there be HCM? What else?
For example: Statistical likelihood that the regular WCT in ECG #1 might be AFlutter ( instead of VT ) is greatly increased in a patient with AFib who is taking Flecainide. The underlying rhythm is AFib ( irregularly irregular QRS without P waves ). Note QRS widening for beats #14-thru-18 in ECG #3.
As per Dr. Smith — this suggests that despite QRS widening, the rhythm in ECG #3 is AFib with a rapid ventricular response. Look next at ECG #5: This rhythm is again irregularly irregular without evidence of atrial activity — so the rhythm is again AFib with a rapid ventricular response. Many of the beats in ECG #3 show extra widening.
I have periodically called attention to examples of the Ashman phenomenon as they occur in Dr. Smith's ECG Blog ( See My Comments in the January 5, 2020 post — the June 17, 2020 post — and the March 30, 2023 post , among others ).
The P EARL — is that when AFib is rapid, parts of the tracing often look regular — but are not truly regular when measured with calipers. P.S. — I believe parts of this tracing represent rapid AFib. Other parts looked to be regular — so I wasn’t sure if there might not be some transition between a regular reentry SVT rhythm and AFib.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content