This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
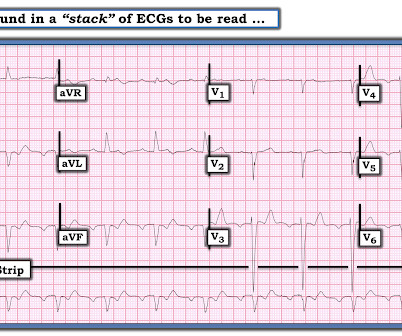
NOTE: The ECG in Figure-1 has been recorded at the usual 25mm/second speed — but with the Cabrera format ( Please see my Editorial Note near the top of the page in ECG Blog #365 for review of the basics of this recording system ). Among the fast Supraventricular Rhythms: This is not AFib — because the rhythm is regular.
A fully upright P-wave is typical atrial activity of atrialflutter as seen in V1. See these example cases of upright P-waves: Case Continued Thus, I was all but certain that this was atrialflutter. IV Digoxin may begin to slow the ventricular response of AFib or AFlutter sooner than many clinicians realize.
To me, it was clearly atrialflutter with 1:1 conduction. The rate of 280 is just right for atrialflutter. The waves look like atrialflutter waves, NOT like a wide ventricular complex. Reverted to atrial fibrillation with RVR while in the hospital 3 times and needed cardioversion.
male with pertinent past medical history including Atrial fibrillation, atrialflutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Now you CAN on occasion see PVCs during reentry SVTs that do not convert the SVT.
Instead, the rate of 150, plus the history of AF, suggested atrialflutter. A close inspection of lead II showed P or flutter waves at a rate of about 300 bpm, also supporting atrialflutter. There appear to be flutter waves at a rate of 300. Flecainide encourages new atrialflutter.
The ECG was interpreted as showing atrialflutter with 2:1 conduction. The heart rate could be compatible with that of a 2:1 conducted atrialflutter. Also, lead I could give the initial impression of showing flutter waves. I have emphasized on many occasions in Dr. Smith's ECG Blog how AFlutter is by far (!)
Jesse McLaren explains his AFIB mnemonic for approach to atrial fibrillation that involves 4 questions: 1. Is it atrial fibrillation? If it is atrial fibrillation and there is rapid ventricular response, is it fast from a secondary cause? Does the patient need an anticoagulant started in the ED?
The WCT is interrupted by a series of variable-morphology QRS complexes, with atrialflutter waves note in II, III, and aVF. Detail of Flutter waves The rate of the flutter waves matches the rate of the WCT (about 200/m), proving that the presenting WCT had been 1:1 atrialflutter.
So this is an extremely slow atrialflutter with 2:1 conduction. Atrial rate 146, ventricular rate 73. I suspect that the amyloid slows the conduction of the atrialflutter. It turned out that he had a history of slow atrialflutter. Atrial arrhythmias ( especially AFib or AFlutter ).
Are the wide complexes due to a supraventricular rhythm (AVNRT or Atrialflutter or atrial fib) with aberrancy? The P EARL — is that when AFib is rapid, parts of the tracing often look regular — but are not truly regular when measured with calipers. P.S. — I believe parts of this tracing represent rapid AFib.
M Y A NSWER: The issue of whether C omputerized E CG I nterpretations are “at fault” for an inaccurate ECG diagnosis has been addressed numerous times on this blog. M Y A NSWER: In my experience, MAT is the 2nd-most commonly overlooked cardiac arrhythmia ( surpassed only by AtrialFlutter ). GET a 12-lead!
The rhythm differential for narrow, regular, and tachycardic is sinus rhythm, SVT (encompassing AVNRT, AVRT, atrial tach, etc), and atrialflutter (another supraventricular rhythm which is usually considered separately from SVTs). Therefore this patient is either in some form of SVT or atrialflutter. If so, why?
There is atrial activity before every QRS, but that activity has negative polarity, so it is not sinus rhythm. There are clearly no flutter waves, so it is not atrialflutter (a "macro-reentrant" atrial tachycardia) Is it AVNRT originating at the superior pole of the AV node, resulting in a retrograde P-wave before the QRS?
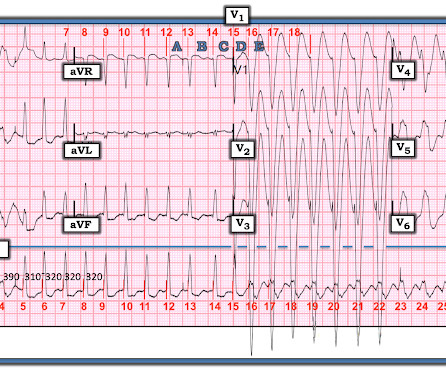
Figure-2: Colored arrows highlight flutter waves , with 2:1 AV conduction. Patient history: It turns out that todays patient is an 80-something year old man with longstanding hypertension and paroxysmal atrial fibrillation. The AFib had been well controlled on Flecainide for many years. VT as a proarrhythmic effect.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content