This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
male with pertinent past medical history including Atrialfibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Description : Regular Wide Complex Tachycardia at a rate of about 160.
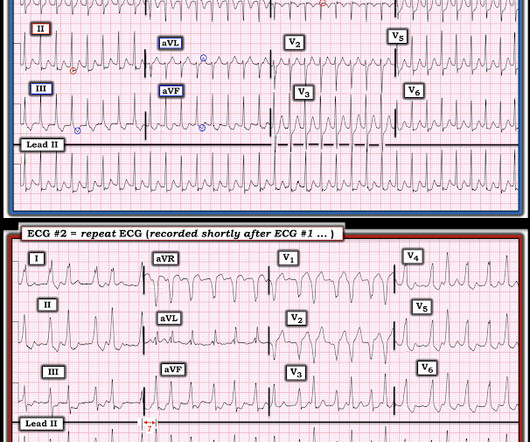
The two ECGs above were texted to me with the text: "Young Guy came in in SVT but now in and out of irregular wide complex tachycardia. -- not sure if polymorphic VT vs. a fib with WPW." Definitely atrialfibrillation. Probably WPW but is very slow for atrial fib withWPW. So this looks like WPW with Atrialfibrillation.
Whenever it is this fast, you need to be very careful to ascertain whether it is irregular ( as in atrialfibrillation with rapid ventricular respsonse ) or regular ( as in VT ). This is not because it is polymorphic VT; it is because it is WPW with atrialfibrillation. Smith : What do you think? It is not VT; it is AF.
Here is the computer interpretation: ATRIALFIBRILLATION WITH RAPID VENTRICULAR RESPONSE WITH ABERRANT CONDUCTION OR VENTRICULAR PREMATURE COMPLEXES LEFT AXIS DEVIATION [QRS AXIS beyone -30] NONSPECIFIC ST and T-WAVE ABNORMALITY The over-reading physician confirmed this diagnosis, which is incorrect. It is not atrialfibrillation.
She also has a hx of paroxysmal atrialfibrillation and is on oral anticoagulant treatment. She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Cardiac output (CO) was being maintained by the tachycardia.
PMH: Known paroxysmal Atrial fib. He is usually is in sinus rhythm as far as he knows, but he cannot subjectively feel atrialfibrillation, so he is never completely certain when he is in sinus or atrial fib. Here is his ECG: Atrial Fib with a Ventricular Response of about 66. He immediately completely recovered.
Detection of Irregular Heart Rhythms Devices such as the Apple Watch or Fitbit Sense can detect irregular heart rhythms, including atrialfibrillation (AFib). These early warnings are critical, as AFib increases the risk of stroke and other heart-related complications.
There were times when it would be usurped by sinus tachycardia, then return to this rhythm. There is no atrial activity to suggest atrialfibrillation. This does NOT seem irregularly irregular enough for AFib … Instead — there is almost “group beating” with “Wenckebach periodicity”. There is a wide complex.
There is a regular wide complex tachycardia. Remember : Adenosine is safe in Regular Wide Complex Tachycardia. Adenosine is only unsafe in atrialfibrillation with WPW , which presents with a very rapid rate, polymorphic QRS, and some very short RR intervals] Bedside echo showed poor LV fct. We want to avoid a stroke.
His previous echo one month prior shows the same thing: “consistent with old infarct in LAD vascular territory, with EF 45%” "I think there is something else causing his tachycardia which is exaggerating his EKG findings and mimicking an acute myocardial infarction." Looks like atrialfibrillation. Cath lab was cancelled.
Wide-complex tachycardia: VT or aberrant, or "other?" The patient had a history of paroxysmal atrialfibrillation and several cardioversions. A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. And indeed the QRS morphology strongly supported VT (e.g. Note of Caution!
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Recently diagnosed with intermittent paroxysmal atrialfibrillation but no EKGs available to confirm. Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Sinus tachycardia does not go this fast.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Atrialfibrillation is also a predictor of worse outcomes in this case (Alborzi). Sinus Tachycardia ( common in any trauma patient. ). He was intubated for altered mental status.
Therefore — the rhythm in ECG #1 is almost certain to be AFib ( A trial F ibrillation ) , seen here with a “rapid” ventricular response. Under normal conditions with AFib — the refractory period of the AV node does not allow more than 150-to-200 impulses/minute to be conducted to the ventricles.
Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered. Nevertheless, the widths of both the QRS complex and the RS duration are similar in both the old ECG and the tachycardia.
Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia. Ventricular tachycardia – more than 7 consecutive complexes originating from ventricles at a rate of > 100 bpm. Supraventricular tachycardia – more than 7 consecutive complexes of supraventricular beats at a rate of > 100 bpm.
Continue reading to learn more about this procedure, its significance in treating atrialfibrillation, and what to expect during treatment. What is AtrialFibrillation? Before diving into electrical cardioversion, we should understand atrialfibrillation (AF). What Is Cardioversion?
The presence or absence of five predetermined cardiac arrhythmias were evaluated: atrialfibrillation/flutter (AFIB), ventricular bigeminy, ventricular trigeminy, ventricular tachycardia (VT), and high-grade atrioventricular block (AVB).Results:The For AFIB, the sensitivity was 0.76 and 0.94, respectively.
ACUTE MI (I allowed Acute MI to be in the report because I knew there would be an elevated troponin from ischemia, which is the definition of acute MI -- but in this case it would most likely be a Type 2 MI from tachycardia) There is also LA-RA lead reversal. The rhythm is rapid AFib. She had some fractures.
The ECG there reportedly showed an irregular tachycardia, and the patient was immediately referred to the emergency room. Here is her ECG on arrival: There is a wide complex tachycardia that is irregularly irregular (this is difficult to determine at these very high rates). Lead aVR seems to show the atrial activity clearly.
Note: Due to the limited number of normally conducted beats — it is hard to be sure whether the underlying rhythm is sinus with baseline artefact or atrialfibrillation. Note: The patient while on telemetry had alternating atrialfibrillation, sinus rhythm with 1st degree AV block and also periods of Wenckebach conduction.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrialfibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. The patient was placed on telemetry.
The collaboration, according to a written statement issued by the company, aims to address challenges in capturing and analyzing cardiac signals to help physicians enhance patient outcomes for atrialfibrillation procedures. 1 Approximately 33 million patients worldwide are living with AFib.
space-line Alcohol and ‘Holiday Heart Syndrome’ Holiday heart syndrome refers to episodes of supraventricular tachycardia: a sudden arrhythmia or irregularity in which the heart beats much faster than normal, explains Dr. Schuitema. Alcohol acts as a natural irritant to the heart muscle, says Dr. Tarditi.
The team immediately paged cardiology, concerned for polymorphic ventricular tachycardia. Since sinus conducted QRS complexes cannot co-exist together with ventricular tachycardia, this must all be artifact. Such as atrialfibrillation or sinus rhythm with extrasystoles. Telemetry Sample 2 Does this change how you feel?
Chart review confirmed that he had been started on flecainide for atrialfibrillation. This new information makes the diagnosis of atrial flutter far more likely: first, atrialfibrillation and flutter are closely associated and, second, this makes a flutter rate of 200 bpm (with 1:1 conduction) quite likely.
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. There is a large peaked P-wave in lead II (right atrial enlargement) There is left axis deviation consistent with left anterior fascicular block. See my quick review of atrialtachycardia below) The tachycardia spontaneously resolved.
The rhythm is atrialfibrillation. I sent it to 2 of my ECG nerd colleagues with no clinical information whatsoever, who instantly said: "Looks like afib with subendocardial ischemia and right heart strain pattern." "I Tachycardia is of course, quite common in patients following cardiac arrest. The rhythm is rapid AFib.
Answer : you must treat the patient's underlying condition causing sinus tachycardia, and repeat the ECG at the lower heart rate. Rate correction should not be used when RR interval has large variability, as in atrialfibrillation. Correlation of QT Interval Correction Methods During AtrialFibrillation and Sinus Rhythm.
Figure-1: While at first glance the rhythm in Figure-1 might be mistaken for sinus tachycardia in fact, this is not the rhythm. Instead there is 2:1 atrial activity that is best seen in lead V1 ( See Figure-2 ). The AFib had been well controlled on Flecainide for many years. Figure-1: The initial ECG in today's case.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content