This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
PEARL # 1: As I emphasize in ECG Blog #148 ( from where I took the tracing I show in Figure-3 ) — the BEST way to prove artifact — is to recognize persistence of an underlying spontaneous rhythm that is unaffected by any erratic or suspicious deflections that are seen. Figure-3: I've reproduced this tracing from ECG Blog #148 ( See text ). =
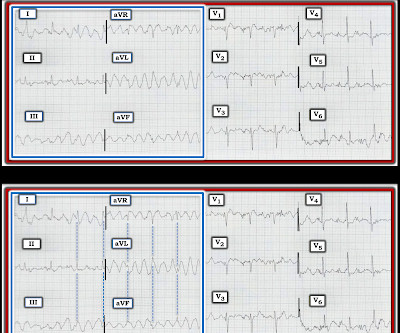
NOTE: The ECG in Figure-1 has been recorded at the usual 25mm/second speed — but with the Cabrera format ( Please see my Editorial Note near the top of the page in ECG Blog #365 for review of the basics of this recording system ). Among the fast Supraventricular Rhythms: This is not AFib — because the rhythm is regular.
This does NOT seem irregularly irregular enough for AFib … Instead — there is almost “group beating” with “Wenckebach periodicity”. Here the full text of the article: Accelerated Idioventricular Rhythm: History and Chronology of the Main Discoveries
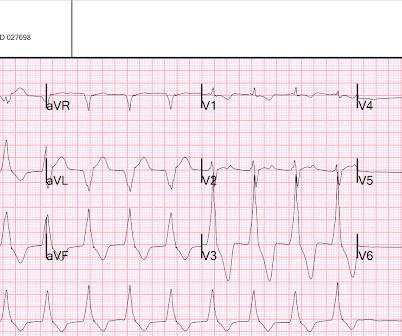
NOTE: The ECGs in today's case are recorded in the Cabrera Format ( See Dr. Grauer Comment in the October 26, 2020 post of Dr. Smith's ECG Blog for review on the Cabrera Format ). KEY Point: Nothing other than AFib with WPW results in a ventricular response this fast ( which is why Figure-2 is pathognomonic for AFib in a patient with WPW ).
As I discussed in detail in My Comment at the bottom of the page in the January 13, 2024 post in Dr. Smith's ECG Blog — pacemaker spikes tend to be a high frequency signal. The April 6, 2023 post — excessive baseline artifact misdiagnosed as AFib ( instead of sinus rhythm with AV Wenckebach — as in Figure-4 in this post ).
. == Links to Examples of ARTIFACT: What follows below is an expanding list of technical "misadventures" — most from Dr. Smith's ECG Blog — some from other sources ( NOTE: As I did not previously keep track of these — there are additional examples of artifact sprinkled through Dr. Smith's ECG Blog that I have not yet included here. ).
Ibutilide can convert atrial fib, or if the atrial fib is resistant to electrical cardioversion, ibutilide can facilitate electrical cardioversion (see my description of the New England Journal article below). I focus my comment on a few additional aspects regarding new AFib. Here is the ECG after ibutilide: What do you notice?
The patient also has a history of AFib and HFmrEF ( = H eart F ailure with M inimally- R educed E jection F raction ). I have emphasized on many occasions in Dr. Smith's ECG Blog how AFlutter is by far (!) Many advances in treatment have occurred in the 28 years since this article was published.
ECG 2 Especially in the context of the first ECG, readers of this blog will readily appreciate the ST elevations and hyperacute T waves in II, III, aVF, V6, and to a lesser extent V5. As discussed on this blog many times before, proportionality is key to the diagnosis of OMI by ECG. [link] I also texted the ECG to Dr. Smith.
This article discusses correction of the QT interval for rate. I've been working on this a long time, thought about submitting it to a journal, but decided it gets more readers on this blog. The article is written by Dr. Smith and Dr. Friedman. In that article, they do not say what is a dangerously short QT is (e.g.
Full text online: [link] Here are excerpts from the article: From the Introduction: Among rhythm diagnoses, atrial fibrillation (AF) is particularly important for appropriate management. AFib is the irregularly irregular rhythm that is most commonly confused with MAT — and , AFib is much, much, much more common than true MAT.
As we've discussed on numerous other posts in Dr. Smith's ECG Blog ( See My Comment at the bottom of the page in the May 5, 2022 post) — a growing number of conditions other than Brugada Syndrome have been found to temporarily produce a Brugada-1 ECG pattern. What are the ECG Findings of Cardiac Contusion?
See this articles: Heart Failure with Preserved Ejection Fraction (NEJM review) One etiology of LVH on the ECG is Hypertrophic Cardiolmyopathy (HOCM), and sometimes ECGs in patients with HOCM are specific for HOCM. WPW Cardiac arrhythmias ( especially AFib ). Abnormal ST-T wave abnormalities. Conduction defects (ie, LBBB, IVCD ).
I focus My Comment on determination of the e tiology of this patient’s tachyarrhythmia — and compare it to other SVT rhythms previously published in Dr. Smith’s ECG Blog. E CG # 2 in Figure-1 is from the October 16, 2019 post on Dr. Smith’s Blog. Unfortunately, that EP study has not yet been done. H eart R ate C an H elp !
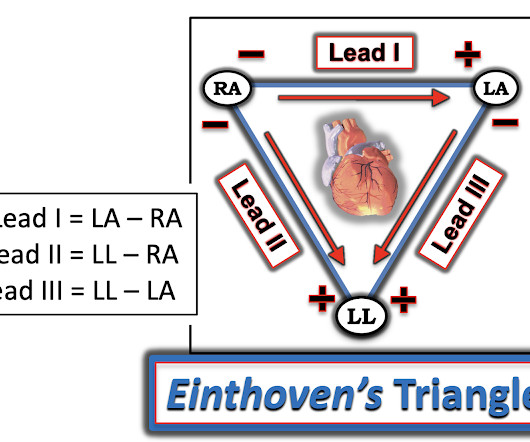
Smith — the fact that artifact in ECG #1 is maximal in leads I and II ( with lead III undistorted ) — points to the RA extremity as the "culprit" ( See My Comment in the December 5, 2022 post of Dr. Smith's ECG Blog for review on how to determine the "culprit" extremity within seconds ). The March 17, 2023 post — for PTA.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content