This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia. Ventricular tachycardia – more than 7 consecutive complexes originating from ventricles at a rate of > 100 bpm. Supraventricular tachycardia – more than 7 consecutive complexes of supraventricular beats at a rate of > 100 bpm.
MY Thoughts on the ECG in Figure-1: When faced with a challenging cardiac arrhythmia — It is a "luxury" to have access to a long lead rhythm strip containing 3 simultaneously -recorded leads. PEARL # 2: When the rate of AFib is rapid — this irregular tachycardia may look regular when it is not.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
Since the patient was stable and tolerating the arrhythmia it was decided to treat with IV Amiodarone for medical conversion. The 2019 ESC Guidelines for the management of patients with supraventricular tachycardia indicated that IV Amiodarone should not be considered in these populations. Smith : What do you think?
Detection of Irregular Heart Rhythms Devices such as the Apple Watch or Fitbit Sense can detect irregular heart rhythms, including atrial fibrillation (AFib). These early warnings are critical, as AFib increases the risk of stroke and other heart-related complications.
His previous echo one month prior shows the same thing: “consistent with old infarct in LAD vascular territory, with EF 45%” "I think there is something else causing his tachycardia which is exaggerating his EKG findings and mimicking an acute myocardial infarction." The patient spontaneously converted back to sinus tachycardia.
Wide-complex tachycardia: VT or aberrant, or "other?" A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. Sinus tachycardia with aberrancy was unlikely as the rate was consistently 150 bpm, without spontaneous variation. And indeed the QRS morphology strongly supported VT (e.g.
There is a regular wide complex tachycardia. Remember : Adenosine is safe in Regular Wide Complex Tachycardia. Rather, from this one: Very Fast Very Wide Complex Tachycardia Ideally, one would cardiovert. PEARL #1: The most commonly overlooked arrhythmia is AFlutter ( A trial F lutter ).
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Is longterm endurance-training a risk factor for AFib and AFlutter? == Why is Today's Initial Rhythm AFlutter? Sinus tachycardia does not go this fast.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ). Sinus Tachycardia ( common in any trauma patient. ). QTc prolongation.
Multifocal Atrial Tachycardia 2. Failure to follow this advice will undoubtedly lead to overlooking subtle acute MIs — and , it will especially lead to misdiagnosing many cardiac arrhythmias ( as was done in this case ). How can you avoid overlooking this arrhythmia? Sinus with multifocal PACs 3. Sinus with multifocal PVCs 4.
Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered. Nevertheless, the widths of both the QRS complex and the RS duration are similar in both the old ECG and the tachycardia.
Therefore — the rhythm in ECG #1 is almost certain to be AFib ( A trial F ibrillation ) , seen here with a “rapid” ventricular response. Under normal conditions with AFib — the refractory period of the AV node does not allow more than 150-to-200 impulses/minute to be conducted to the ventricles.
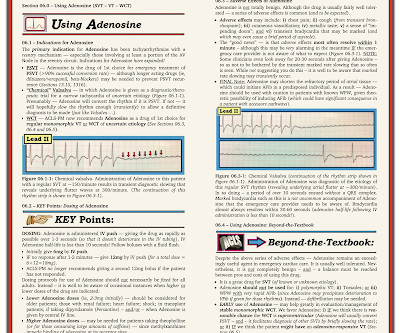
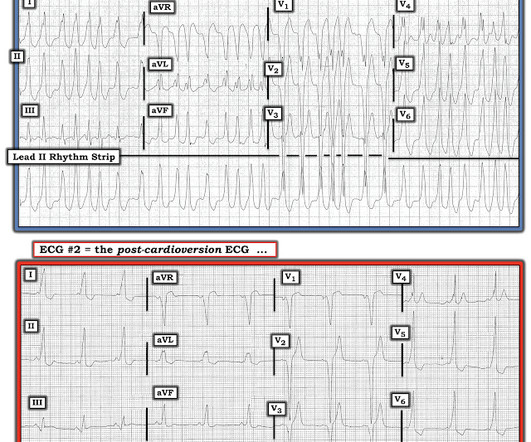
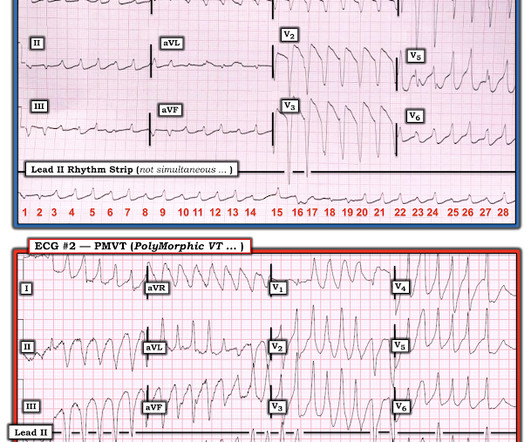
MY THOUGHTS on ECG #1: My initial impression on looking at the ECG in Figure-1 — was that the rhythm was either rapid AFib in a patient with WPW — or — PMVT ( P oly M orphic VT ). The reason I initially thought the underlying rhythm was AFib — is that no atrial activity is seen in any lead and the rhythm “looks” irregular. See text ).
during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. The easy way to remember the arrhythmias most commonly associated with SSS is to think of what one might expect if the SA node became sick. New slow AFib reflects a combination of these rhythm problems. second in duration.
The finding of a fairly regular, wide tachycardia without clear sign of atrial activity ( especially when seen in an acutely symptomatic patient ) — should immediately prompt a diagnosis of VT until proven otherwise. These findings suggest that instead of VT — the rhythm in Figure-1 is AFib with a fairly rapid ventricular response.
The presence or absence of five predetermined cardiac arrhythmias were evaluated: atrial fibrillation/flutter (AFIB), ventricular bigeminy, ventricular trigeminy, ventricular tachycardia (VT), and high-grade atrioventricular block (AVB).Results:The For AFIB, the sensitivity was 0.76 for the AI platform compared to 0.74
Because of this, it is uncommon to see sinus tachycardia with a prolonged PR interval. P utting I t A ll T ogether: At this point in my assessment of today's rhythm — I fully acknowledge that I did not know for certain the etiology of this arrhythmia. Figure-3: How to assess for possible 2:1 atrial activity. =
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( How would YOU interpret this tracing? How to manage the patient?
I was sent the ECG shown in Figure-1 — being told only that providers on the case suspected AFib ( A trial Fib rillation ) with RBBB ( R ight B undle B ranch B lock ) aberrancy. QUESTIONS: Is the wide tachycardia that is seen best in the chest leads, too irregular to be VT ( V entricular T achycardia )? —
The ECG there reportedly showed an irregular tachycardia, and the patient was immediately referred to the emergency room. Here is her ECG on arrival: There is a wide complex tachycardia that is irregularly irregular (this is difficult to determine at these very high rates). Vitals were within normal limits other than heart rate.
Cardioversion is used to correct abnormal heart rhythms, also known as arrhythmias. Electrical cardioversion may be recommended for you if you have certain types of arrhythmias, such as: Atrial fibrillation (AFib): This is the most common type of arrhythmia, and it can cause symptoms like dizziness, fatigue, and difficulty breathing.
Learning points : Takotsubo can lead to cardiac arrest from ventricular arrhythmia. But there are 3 other wide beats in the tachycardia that begins with beat #6 ( = beats #7; 13,14 ). The QTc then gradually shortened over the course of several days as is usual for stress cardiomyopathy.
What is unusual about this arrhythmia? Doing so suggests that the R-R interval of this exceedingly rapid arrhythmia is just a tiny amount over 1 large box — which corresponds to a ventricular rate just under 300/minute ( ie, between 290-300/minute ). How would YOU interpret the ECG in Figure-1 ?
He has a family history concerning for arrhythmia. Given the circumstances of his car crash, we presume it was due to an underlying arrhythmia. He has a family history concerning for arrhythmia with his father requiring some sort of device (PPM, ICD, unclear) at a young age.
PEARL #2: As cited in ECG Blog #252 — my favorite truism in arrhythmia interpretation is, "The commonest cause of a pause is a blocked PAC". ECG Blog #71 — Regarding the Ashman Phenomenon with AFib. The September 30, 2019 post in Dr. Smith’s ECG Blog — for an example of “MAT”, but without the tachycardia.
With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Systematic Assessment of the ECG in Figure-1: My Descriptive Analysis of ECG findings in Figure-1 is as follows: Sinus tachycardia at ~110/minute. The patient had mild but diffuse abdominal tenderness.
Volta Medical has announced it has entered into a Joint Development Agreement with GE Healthcare to enhance arrhythmia procedures with artificial intelligence (AI)-driven electrophysiology technologies. 1 Approximately 33 million patients worldwide are living with AFib.
In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished. 2) Tachycardia to this degree can cause ST segment changes in several ways. Sometimes what appears to be thrombus on angiogram is not actually thrombus.
space-line Alcohol and ‘Holiday Heart Syndrome’ Holiday heart syndrome refers to episodes of supraventricular tachycardia: a sudden arrhythmia or irregularity in which the heart beats much faster than normal, explains Dr. Schuitema. Alcohol acts as a natural irritant to the heart muscle, says Dr. Tarditi.
Initial vital signs include: NIBP 99/58 HR 150-160 (trend) RR 10 (spontaneous, but shallow) SpO2 86 (RA) BBS CTA The initial rhythm strip is attached: Figure 1 There is a wide complex tachycardia of varying morphology, amplitude, and R-R cycle length. The rS configuration in Lead I displays a persistent rightward axis.
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. An ECG was recorded: This shows a regular narrow complex tachycardia at a rate of about 160. See my quick review of atrial tachycardia below) The tachycardia spontaneously resolved. BP:143/99, Pulse 109, Temp 37.2 °C
We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW.
See this even more interesting and more dramatic and fascinating case: History of Hypertrophic Cardiomyopathy (HOCM), with Tachycardia and High Lactate = My Comment by K EN G RAUER, MD ( 10/28 /2023 ): = QUESTION: For clarity in Figure-1 — I've reproduced today's ECG without the long lead rhythm strip. Abnormal ST-T wave abnormalities.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content