This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The PROACT study reported no impact on cardiotoxicity biomarkers or secondary endpoints related to heart function among patients who took high doses of enalapril, an ACEinhibitor, along with high doses of anthracyclines. The mean dose of enalapril among those who were randomized to take the ACEinhibitor was 17.7mg.
Most people with high blood pressure will be treated with an ACEinhibitor, ARB, calcium channel blocker or a diuretic. Outcome over process, in my view, works best here. There is a range of blood pressure-lowering medications available. There are others also. Hypertension. N Engl J Med. 2015 Nov 26;373(22):2103-16.
This includes beta-blockers, ACEinhibitors, ARBs, ARNIs, MRAs, and SGLT2 inhibitors. The primary outcome is the GDMT prescription rate score, with secondary outcomes covering the time to full GDMT optimization, patient and clinician satisfaction, time spent on healthcare, and the Kansas City Cardiomyopathy Questionnaire.
In fact, a 2024 report on heart failure trends and outcomes published in the Journal of Cardiac Failure showed that in patients with heart failure with preserved ejection fraction, 5-year mortality was 75.7%. Heart Failure Epidemiology and Outcomes Statistics: A Report of the Heart Failure Society of America. 4 Approximately 6.7
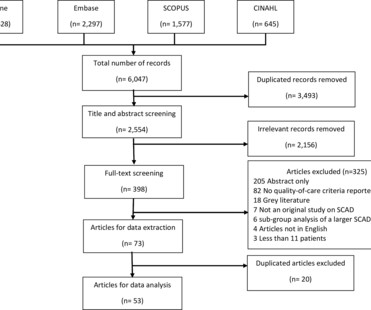
received ACEinhibitors or aldosterone receptor blockers (ACEIs/ARBs), 54.4% (CI 45.4 Raising awareness about consensus recommendations and further prospective evidence about their effect on outcomes may help improve the quality of care for these patients. On random effects meta-analysis, 92.1% (95% CI 89.3
Additionally, exercise-induced hypertension and masked hypertension contribute to adverse outcomes. Oral beta-blockers, ACEinhibitors (ACE-Is), angiotensin receptor blockers (ARBs) and calcium channel blockers (CCBs) are most commonly used for chronic hypertension.
Researchers tracked outcomes for a median of just under 18 months. All secondary endpoints related specifically to heart failure outcomes were significantly reduced among patients who received empagliflozin. The study’s primary composite endpoint occurred in 8.2% of those who received empagliflozin and 9.1% of the control group.
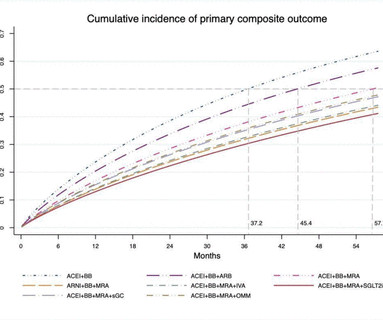
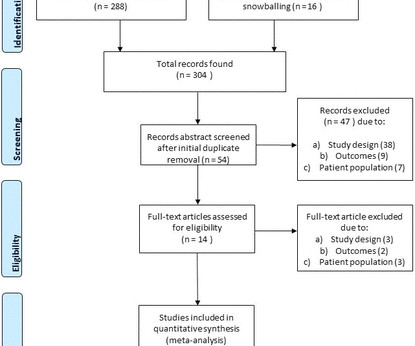
A network meta-analysis aimed to compare effects of both conventional and alternative drug combinations on time to develop primary composite outcome of cardiovascular death or heart failure hospitalisation (PCO). Methods Randomised controlled trials (RCTs) were identified from Medline, Scopus up to June 2021.
Renin–angiotensin system (RAS) inhibitors could potentially improve cardiac remodelling and clinical outcomes after SAVR. The primary outcome was major adverse cardiovascular events (MACEs; all-cause mortality, stroke or myocardial infarction). Both treatment with ACEinhibitors (aHR 0.89 (95% CI 0.82
Researchers tracked outcomes for a median of just under 18 months. All secondary endpoints related specifically to heart failure outcomes were significantly reduced among patients who received empagliflozin. The study’s primary composite endpoint occurred in 8.2% of those who received empagliflozin and 9.1% of the control group.
The aim of this study was to evaluate in a network meta-analysis if beta-blockers (BB) and ACEinhibitors/angiotensin receptor blockers (ACEi/ARBs), in combination or not, can effectively prevent TTS recurrences. The primary outcome was TTS recurrence.
ACEInhibitors WHAT THEY DO : ACEinhibitors block the angiotensin-converting enzyme (ACE) which causes narrowing of blood vessels. COMMON NAMES : Some common brand name ACEinhibitor drugs available to patients with CHD include lisinopril, ramipril and enalapril.
were on ACEinhibitors/angiotensin receptor blockers and 54.9% Sociodemographic characteristics also played a role on the outcome, which can be targeted when planning interventions to improve outcomes. Results A total of 237 participants were included in the final analysis. The mean age was 61.3±17.36
Methods and results Patients ( n = 5661) included in the PARADISE MI trial (Prospective ARNI vs. ACEInhibitor Trial to Determine Superiority in Reducing Heart Failure Events After MI) were stratified according to MRA. Primary outcomes in this substudy were worsening heart failure or cardiovascular death.
These trials added weight to the evidence that supported the use of both angiotensin-converting enzyme inhibitors (ACEi) or ARBs in diabetic kidney disease and chronic kidney disease (CKD), particularly in patients with proteinuria.
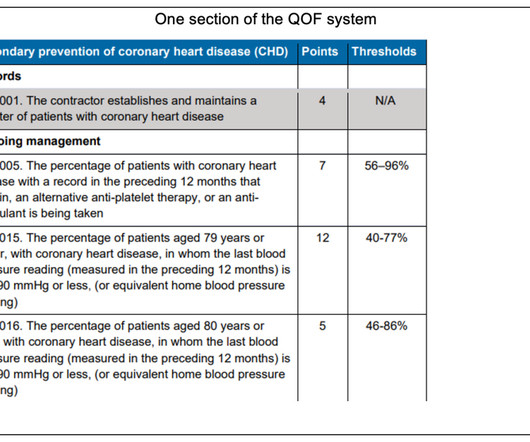
20th October 2023 (With lessons from, and for, all other health services around the world) The Quality and Outcomes Framework The Quality and Outcomes Framework (QOF) was to be the glittering triumph of Evidence Based Medicine. Many of the commonest and most deadly diseases afflicting humanity would be picked up early, then treated.
associated typical Myocardial Infarction therapies such as statins and ACEinhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. Lindahl et al. References: 1. Lindahl B, Baron T, Erlinge D, et al.
If we are unable to build a relationship of trust with the patient then we are going to fail in achieving the best outcome for that patient and this is why engagement and empathy are so essential. Secondly all management should be ensconced in kindness, patience, connection and good communication.
associated typical Myocardial Infarction therapies such as statins and ACEinhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. Lindahl et al. References: 1. Lindahl B, Baron T, Erlinge D, et al.
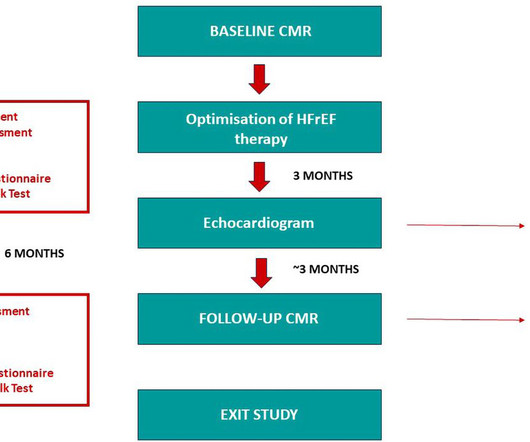
Methods HFrEF patients with symptomatic LVEF≤35% despite ACEinhibitor/beta blocker/mineralocorticoid receptor antagonist therapy, and qualified for sacubitril/valsartan switchover were recruited to this single centre prospective study. Clinical, volumetric and outcome data were collected and compared.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content