This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The PROACT study reported no impact on cardiotoxicity biomarkers or secondary endpoints related to heart function among patients who took high doses of enalapril, an ACEinhibitor, along with high doses of anthracyclines. The mean dose of enalapril among those who were randomized to take the ACEinhibitor was 17.7mg.
Curtain etal1 performed an analysis of the VALIANT (Valsartan in Acute Myocardial Infarction) and PARADISE-MI (Prospective ARNi vs ACEInhibitor Trial to Determine Superiority in Reducing Heart Failure Events After MI) trials to evaluate whether risk of sudden cardiac arrest (SCA) following acute myocardial infarction (MI) has changed over time.
Can patients with advanced chronic kidney disease (CKD) be initiated on angiotensin-converting enzyme inhibitors (ACEi) or angiotensin-receptor blockers (ARBs) without increasing their risk for needing kidney failure replacement therapy?
Most people with high blood pressure will be treated with an ACEinhibitor, ARB, calcium channel blocker or a diuretic. 6 Mortality and Morbidity Among Individuals With Hypertension Receiving a Diuretic, ACEInhibitor, or Calcium Channel Blocker: A Secondary Analysis of a Randomized Clinical Trial. There are others also.
This secondary analysis of the Valsartan in Acute Myocardial Infarction (VALIANT) and Prospective ARNi vs ACEInhibitor Trial to Determine Superiority in Reducing Heart Failure Events After MI (PARADISE-MI) randomized clinical trials investigates the changes over time in sudden death rate after myocardial infarction and the characteristics of people (..)
The goal of the PARADISE-MI trial was to assess the efficacy and safety of sacubitril/valsartan compared with ramipril in a contemporary acute myocardial infarction (AMI) population.
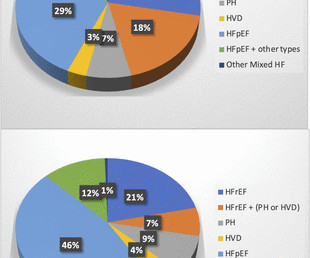
This includes beta-blockers, ACEinhibitors, ARBs, ARNIs, MRAs, and SGLT2 inhibitors. The 2021 European Society of Cardiology guidelines recommend guideline-directed medical therapy (GDMT) for patients with HF with reduced ejection fraction (HFrEF).
Capoten (captopril) is an ACEinhibitor. The Patient: Unfortunately, this is an old tracing, and we do not have patient information, other than the list of medications the patient has been taking, (Lasix, Capoten, Ntg, and Procardia). Lasix (furosemide) is a potassium – wasting diuretic.
A Study to Learn More About How Well the Study Treatment Finerenone Works, How Safe it is, How it Moves Into, Through and Out of the Body, and the Effects it Has on the Body When Taken With an ACEInhibitor or Angiotensin Receptor Blocker in Children with Chronic Kidney Disease and Proteinuria (FIONA). Clinical trial registration No.
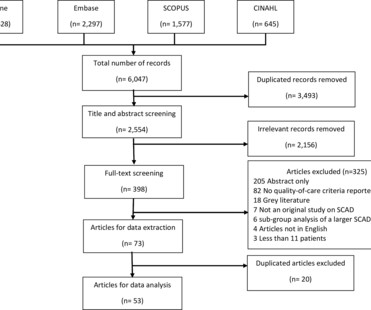
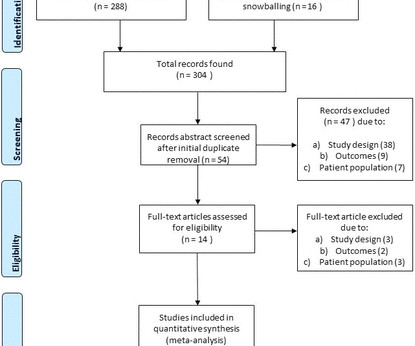
received ACEinhibitors or aldosterone receptor blockers (ACEIs/ARBs), 54.4% (CI 45.4 On random effects meta-analysis, 92.1% (95% CI 89.3 received at least one antiplatelet, 78.0% (CI 73.5 received beta-blockers, 58.7% (CI 52.3 were screened for fibromuscular dysplasia (FMD), and 70.2% (CI 60.8
Common medications include diuretics, ACEinhibitors, beta-blockers, and calcium channel blockers. Follow Your Doctors Advice : If lifestyle changes arent enough, your doctor may prescribe medications to manage your blood pressure.
Publication date: Available online 7 August 2024 Source: The American Journal of Cardiology Author(s): Johanna A. van der Zande, Karishma P. Ramlakhan, Katja Prokselj, Edison Muñoz-Ortiz, Amalia Baroutidou, Magdalena Lipczynska, Edit Nagy, Tobias Rutz, Arie Franx, Roger Hall, Mark R. Johnson, Jolien W. Roos-Hesselink, ROPAC investigators
Resistant hypertension is a condition where blood pressure levels remain elevated above target despite changes in lifestyle and concurrent use of at least three antihypertensive agents, including a long-acting calcium channel blocker (CCB), a blocker of the renin-angiotensin system (ACEinhibitor or angiotensin receptor blocker) and a diuretic.
Time-updated adjusted Cox regression models were used to compare patients with and without RAS inhibitors. Subgroup analyses were performed, as well as a comparison between angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs). Both treatment with ACEinhibitors (aHR 0.89 (95% CI 0.82
were on a beta blocker and on an ACEinhibitor/angiotensin receptor blocker/angiotensin receptor-neprilysin inhibitor, respectively. During the second period, and following the consultation, of the patients with HF with reduced ejection fraction (HFrEF), 86.4%
ACEInhibitors WHAT THEY DO : ACEinhibitors block the angiotensin-converting enzyme (ACE) which causes narrowing of blood vessels. COMMON NAMES : Some common brand name ACEinhibitor drugs available to patients with CHD include lisinopril, ramipril and enalapril.
Medications Medications are often the first line of treatment for cardiomegaly and can include: ACEinhibitors or ARBs , which help lower blood pressure and reduce the workload on the heart. The primary goals of treatment are to address the root cause, reduce the heart’s workload, and prevent complications like heart failure.
The aim of this study was to evaluate in a network meta-analysis if beta-blockers (BB) and ACEinhibitors/angiotensin receptor blockers (ACEi/ARBs), in combination or not, can effectively prevent TTS recurrences. Recurrences of TTS are not infrequent and there is no standard preventive therapy.
In silico analysis of FDA-approved drugs led to the identification of an ACEinhibitor, ramipril, that protected against sunitinib-induced vascular dysfunction in vitro and in vivo, all while preserving the efficacy of cancer therapy.
At multivariable analysis, smoking habit (OR 2.28; p<0.0001), history of traumatic syncope (OR 2.29; p=0.0001) and ACEinhibitors/angiotensin II receptor blockers (OR 4.74; p<0.0001) were independently associated with SS. Patients with SS were older (48.8±20.0 ±20.0 ±19.1, vs 47.7%, p=0.001).
Twenty years ago, Wald and Law 1 hypothesised that, if a combination pill could be made including aspirin, folic acid, a statin, and a low-dose diuretic, beta blocker and angiotensin-converting enzyme (ACE) inhibitor (thus, allowing for the simultaneous modification of four different risk factors: low-density lipoprotein [LDL]-cholesterol, blood pressure, (..)
White with interaction by prevalent stroke status, adjusted for demographic and socioeconomic status.Results:Of 17,222 participants without prevalent stroke at Visit 1, Black participants had greater odds of ACE-inhibitor usage relative to White participants (OR 1.68, 95% CI 1.44-1.95).
Those with sinus tachycardia were treated with beta-blockers and those with ventricular hypertrophy received a beta-blocker and ACE-inhibitor combination. This provided comprehensive rhythm surveillance and automatic downloads of all detections to a monitoring station for cardiology interpretation.
Cardiac MRI did not show significant ischemic findings.The patient received medical therapy consisting of antiplatelet agents, high dose statin, beta blocker and ACEinhibitor, as well as diuretics. Notably, the LAD had multiple aneurysmal segments and areas of eccentric stenosis upto 90%.Multislice
were on ACEinhibitors/angiotensin receptor blockers and 54.9% Results A total of 237 participants were included in the final analysis. The mean age was 61.3±17.36 years, and the majority (57.8%) were male participants. on beta-blockers.
Methods and results Patients ( n = 5661) included in the PARADISE MI trial (Prospective ARNI vs. ACEInhibitor Trial to Determine Superiority in Reducing Heart Failure Events After MI) were stratified according to MRA. Primary outcomes in this substudy were worsening heart failure or cardiovascular death.
Women received more discharge cardiac medications than men: antiplatelet agents, statins, beta blockers, ACEinhibitors, angiotensin II blockers, calcium channel blockers, and nitrates (p=0.0002 - 0.04).Follow-up Length of stay (LOS) in the CPU to discharge was 10.4
ACEinhibitors block the angiotensin-converting enzyme to reduce blood pressure. Defining an exercise pill Experts who have commented on the idea of an exercise pill note one glaring issue: the term “exercise mimetic” is a not only a misnomer, but it’s inaccurate and misleading. Statins lower cholesterol.
ACEinhibitors, or potassium-sparing diuretics), are particularly susceptible. A brief review of the pathophysiology of hyperkalemia will help set the stage for the ECG changes inherent therein. Other causes include metabolic acidosis, in which hydrogen ions shift into the cells in exchange for potassium.
ACEinhibitors, or potassium-sparing diuretics), are particularly susceptible. This ECG is pathognomonic for hyperkalemia. Predisposition to hyperkalemia is complex, but in general, patients with renal disease, or those taking medications that yield potassium retention (e.g.
associated typical Myocardial Infarction therapies such as statins and ACEinhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. Lindahl et al.
Whilst we had evidence (from drug company sponsored clinical trials) demonstrating that certain actions e.g., taking an ACE-inhibitor after a heart attack, reduced the risk of future heart attacks. I had many concerns, but I will just stick to one here. Or, if the interactions between all four drugs might cancel out any benefit.
These include ACEinhibitors (medications such as ramipril, lisinopril, perindopril etc), beta-blockers (carvedilol, Bisoprolol, nebivolol), aldosterone antagonists (spironolactone), Entresto and now there is a new class of medications called SGLT2 inhibitors such as Dapagliflozin.
The patient stated he had a long history of well-controlled hypertension for which he was compliant with his ACE-inhibitor. His pain radiated to his shoulders throughout the evening and the night but it did not prompt him to seek medical attention. He was also treated for erectile dysfunction but had not taken any medications recently.
We now do have some really good medications that help do both and these include: ACEInhibitors/Entresto Beta Blockers MRAs – Mineraloreceptor antagonists SGLT2 inhibitors And ideally anyone with heart failure should be on all these medications unless they are intolerant or in some way the medications are contraindicated.
“In spite of the accumulating evidence of their efficacy, established treatments for maintaining renal function remain woefully underutilized. Clinicians and health care systems must be encouraged to make use of these treatments.”
These include ACEinhibitors (and now a medication called Entresto), beta blockers, Mineralocorticoid receptor antagonists and now a new class of anti-diabetic medications called SGLT2 inhibitors and ideally wherever possible the patient should try and take a little of all of them as opposed to taking lots of one and none of the others.
associated typical Myocardial Infarction therapies such as statins and ACEinhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. Lindahl et al.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content