This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Opiates are associated with worse outcomes in Myocardial Infarction. Cath attending is aware.
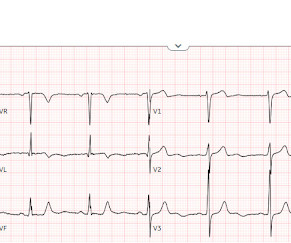
Written by Jesse McLaren Three patients presented with acute chest pain and ECGs that were labeled by the computer as completely normal, and which was confirmed by the final cardiology interpretation (which is blinded to patient outcome) also as completely normal. What do you think?
This was a machine read STEMI positive OMI. the investigators reviewed outcomes in 118 patients presenting with NSTEMI. The meaning of this quote is that at times, something as obvious as the dramatic anterior lead ST elevation that we see in today's tracing is not the result of an acute LAD STEMI. His ECG is shown below.
See this post: Septal STEMI with ST elevation in V1 and V4R, and reciprocal ST depression in V5, V6. After being transferred to an academic center, she was taken to the cath lab: Proximal RCA occlusion (causing inferior and RV OMI) Unfortunately, she continued to decline despite aggressive measures. Also seen in inferior + RV OMI.)
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Immediate versus delayed invasive intervention for non-stemi patients. Academic Emergency Medicine 27(S1): S220; May 2020.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. Long term outcome unknown but obviously bleak.
There is an obvious inferior posterior STEMI(+) OMI. We recorded an ECG in which V1-V3 were put in the position of V4R-V6R, and V4-6 were placed in V7-9 to (academically) confirm posterior OMI. I say academically because the STD in V2 is diagnostic -- posterior leads are NOT necessary. What is the atrial activity? What to do?
It is a sad academic story ,most of the interventional cardiology community shrugged it off as a non-event. No one knows how the pPCI related delay was legally ratified and academically accepted by the elite cardiology forums. best, It has a miniscule 1 % edge in the outcome if performed on time, at a expertise intensive place.
Still , even today it is weird to see hours of academic time is consumed in CTO Interventions in any interventional cardiology meets. Periprocedural and clinical outcomes of percutaneous coronary intervention of chronic total occlusions in patients with low- and mid-range ejection fractions. Surprise… surprise !, Life (Basel).
It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. Could there have been a different outcome if the crews immediately recognized OMI – versus a shortened PR-interval – and commenced with pre-hospital Cath Lab activation? Is this OMI?
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. Is that an obvious STEMI underneath that rhythm? Again, not an expected outcome with diltiazem). Is this inferor STEMI? Atrial Flutter with Inferior STEMI?
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). Yet this is rarely followed, and patient outcomes like this are the result once in a while.
Immediate and early percutaneous coronary intervention in very high-risk and high-risk Non-STEMI patients. Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. Academic Emergency Medicine 27(S1): S220. Unfortunately, they follow their own guidelines only 6% of the time!!
He has a history of coronary artery disease and a STEMI two years prior that was treated with primary PCI. At the time of this initial ED ECG, his symptoms were improving ECG #1 on admission to the ED The patient was not seen quickly in the ED as it was a busy shift and the ECG did not meet STEMI criteria. The below ECG was recorded.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content