This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Ischaemic events were defined as myocardialinfarction, stroke, transient ischaemic attack or peripheral embolism at 1 year. Bleeding events were defined as any bleeding based on the Valve Academic Research Consortium-2 consensus document at 1 year.
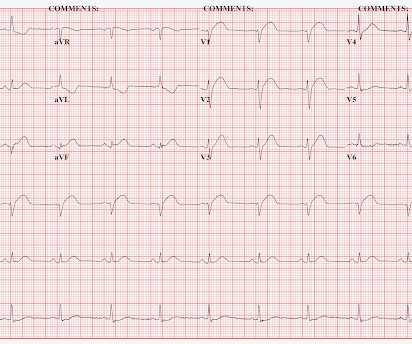
We recorded an ECG in which V1-V3 were put in the position of V4R-V6R, and V4-6 were placed in V7-9 to (academically) confirm posterior OMI. I say academically because the STD in V2 is diagnostic -- posterior leads are NOT necessary. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. What to do?
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. A New ST-segment elevation myocardialinfarction equivalent pattern? Academic Emergency Medicine 27(S1): S220; May 2020.
He was found to have a 100% circumflex lesion for which a bare metal stent was placed. Academic Emergency Medicine 24(1):120-124. The Comparison of Physician to Computer Interpreted Electrocardiograms on ST-elevation MyocardialInfarction Door-to-balloon Times. It is not subtle any more. References : 1. Hug hes KE.,
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardialinfarction, or any prior PCI/stent. No appreciable skin pallor. He reported to be a social drinker, but used tobacco products daily. Here is the time-zero 12 Lead ECG.
Occlusion myocardialinfarction is a clinical diagnosis Written by Willy Frick (@Willyhfrick). Here is the angiogram after stent placement. The patient suffered a large infarct. St depression in lead AVL differentiates inferior st-elevation myocardialinfarction from pericarditis. Circulation , 130 (25).
Association between opioid analgesia and delays to cardiac catheterization of patients with occlusion MyocardialInfarctions. Academic Emergency Medicine 27(S1): S220. A single DES stent was placed, and the patient did well post-procedure. Abstract 556. Most other arteries had scattered 20-30% stenoses.
Stone, MD Mount Sinai Health System tim.hodson Wed, 04/02/2025 - 15:26 March 31, 2025 Using intravascular imaging (IVI) to guide stent implantation during complex stenting procedures is safer and more effective for patients with severely calcified coronary artery disease than conventional angiography, the more commonly used technique.
Patients with ST-segment–elevation myocardialinfarction undergoing primary percutaneous coronary intervention were randomly assigned by center to receive low-dose PPA or matching placebo for at least 48 hours. Circulation, Ahead of Print. mg·kg·h of bivalirudin intravenously). mg·kg·h of bivalirudin intravenously).
Drug‐eluting stents have been shown to be superior to bare‐metal stents in patients with HBR, even when patients were given abbreviated periods of dual antiplatelet therapy (DAPT). Short DAPT has not been evaluated with the EluNIR ridaforolimus‐eluting stent. presented with acute coronary syndrome; 33.7%
Doctors then treat the cause of the heart attack, either inserting a stent, removing a clot or taking other necessary action. The NCSI study involved cardiologists at both community hospitals, where many patients with heart attack first present, and large academic centers. Division Head of Cardiology at Henry Ford Health.
3.30]) and subacute definite or probable stent thrombosis (0.58% and 0.17%; hazard ratio, 3.40 [95% CI, 1.26–9.23]) mg/day) monotherapy or to DAPT with aspirin (81–100 mg/day) and prasugrel (3.75 mg/day) after loading of 20 mg of prasugrel in both groups. years; men, 76.6%; acute coronary syndrome, 75.0%).
The primary outcome was major adverse cardiac and cerebrovascular event (MACCE), namely a composite of death from cardiovascular causes, myocardialinfarction (MI), stroke, stent thrombosis within 12 month. The secondary outcome was Bleeding Academic Research Consortium (BARC) scale bleeding events within 12 months.
EMPACT-MI 1 ( NCT04509674 ) studied the effects of empagliflozin in patients who have experienced myocardialinfarction (MI). The primary superiority endpoint was clinically relevant bleeding (Bleeding Academic Research Consortium [known as BARC] types 2, 3, or 5). Here is our curated list of the top sessions. April 6, 2024.
I limit my comments to a number of academic and semantic concepts relating to the arrhythmia in this case: What is an “SVT”? Serial troponin T measurements rose from zero to 2.80 ng/mL over the next 10 hours. Here is the ECG after intervention: Persistent STE in III and aVF, with persistent STD in V2-V5.
In their haste to hyperventilate about MINOCA, the authors don’t highlight the high percentage of cardiac interventions that are needed in patients with conventional, common epicardial disease - 80% need a coronary stent and 10% need open heart surgery. But these are words you won’t find in the chest pain guidelines of 2023.
History of diabetes type II and stent placement in 2018. Let's see how the PMCardio Queen of Hearts AI Model performs: "Acute Occlusive MyocardialInfarction" She gave this a score of 1.0 (100% This was texted to me by a paramedic while I was out running one day: "54 yo male chest pain started at 1pm. What do you think?
ECG #3 is easily recognized as OMI and the AI model recommends immediate revascularization The patient in today's case received suboptimal care and suffered a substantial myocardialinfarction. He eventually underwent CAG, where a circumflex occlusion was stented. Academic Emergency Medicine 27(S1): S220; May 2020.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content