This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished. First , there can simply be diffuse ST depressions (which obligates reciprocal STE in aVR) associated with tachycardia which are not indicative of ischemia.
Final diagnosis of cerebral ischemia was made in 662/1043 patients (63.5%) and stroke mimic was diagnosed in 381/1043 patients (36.5%). Detailed chart review was conducted to extract both the variables needed to apply the mimic scales the final diagnosis confirmed by final imaging and discharge diagnosis (cerebral ischemic vs stroke mimic).
Dr. Stone is Director of Academic Affairs for the Mount Sinai Health System and Professor of Medicine (Cardiology) and Professor of Population Health Science and Policy at the Icahn School of Medicine at Mount Sinai, and the study chair of the ECLIPSE trial. These results extend the strong recommendations from recent U.S.
In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. Remember that the RV is the most anterior chamber. Here is a transverse image of a CT showing this. A few clues that might have suggested this are: There is marked STE in V1.
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. This rules out subendocardial ischemia and is diagnostic of posterior OMI. V4-5 continue to show STD.
Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. and repeat the ECG, to see if the apparent ischemia persists. A third ECG was done about 25 minutes after the first: This shows resolution of all apparent ischemia.
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia.
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). There is STE in aVR. Thus, there is high lateral OMI with diffuse ST depression. Moreover, left main occlusion often presents near death.
There is no definite evidence of acute ischemia. (ie, Distinction of PMVT vs VFib is an academic one in this case ). Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. ( Some residual ischemia in the infarct border might still be present.
Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. This distinction is more than academic — because both treatment and the response to therapy tend to be different with these 2 entities. Acute ischemia? Case continued The tachyarrhythmia terminated on its own. g IV dose of Magnesium.
V1 sits over both the RV and the septum, so transmural ischemia of either one with give OMI pattern in V1 and reciprocal STD in V5 and V6. After being transferred to an academic center, she was taken to the cath lab: Proximal RCA occlusion (causing inferior and RV OMI) Unfortunately, she continued to decline despite aggressive measures.
A combined effort from academic investigators, industry, and regulators is needed to improve imaging technologies and, ultimately, patient outcomes. Imaging in acute ischemic stroke treatment has advanced significantly, but important challenges remain that need to be addressed.
So, we desperately required to break this inappropriate menace with evidence base like COURAGE, ISCHEMIA, BARI-2D, These studies tried to apply some breaks, but the force was weak and couldn’t abolish a pseudo-academic vice. There seems to be a non-academic indication for doing this study to undo the damage done by ORBITA-1.
Objective:To assess whether diffusion restriction (DR) of the retina and optic nerve (ON) can be accurately and reliably identified on standard stroke protocol brain magnetic resonance diffusion-weighted imaging (DWI-MRI) in patients presenting with acute non-arteritic central retinal artery occlusion (CRAO).Background:Retinal
There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). Academic Emergency Medicine 27(S1): S220; May 2020. I sent the last one to the Queen of Hearts #PMCardio app and here is the verdict: My response: "It’s not even subtle.
Smith : the profound persistent STE suggests either persistent occlusion or " no reflow " with persistent downstream ischemia. It makes you think you have done something for the ischemia when you have not! Academic Emergency Medicine 27(S1): S220; May 2020. Setting – large, academic, suburban ED. Abstract 556.
The COMPARE 60/80 HBR trial is the first randomized clinical trial conducted after the release of the ARC HBR (Academic Research Consortium for High Bleeding Risk) guidelines, enrolling only HBR patients as defined by these criteria.
I do not think this ECG is by itself diagnostic of OMI (full thickness, subepicardial ischemia ), b ut comparison to a previous might reveal this ECG as diagnostic of OMI. Academic Emergency Medicine 27(S1): S220. Smith comment: There is a change in V2 as well, with less normal STE and a smaller T-wave with some inversion.
Traditional methods of non-invasive ischemia testing (stress EKG , stress echo, SPECT , PET , direct-to-cath) can result in false negatives 20-30 percent of the time, which can lead to undetected disease, and false positives over 50 percent of the time, which can lead to unnecessary invasive procedures.
It does not usually represent subendocardial ischemia, but rather it is usually reciprocal ST depression, reciprocal to inferior ST elevation. The generalities stated here for predicting ischemia are much more likely to apply when other factors are minimal. Had episode of nausea and dizziness when it started. Sounds like reflux, right?
There was no evidence of ischemia. In the interest of academic discussion Ill present a nother p erspective on selected aspects this case. We are not told how ischemia has been ruled out in this case. They clearly do not s uggest acute coronary occlusion but they are consistent with ischemia. Hyperkalemia.
The ECG is diagnostic of LAD occlusion (or even left main occlusion possibly), with the classic pattern of RBBB and LAFB with huge concordant STE in V1-V2, I, and aVL, with reciprocal depression in most other leads (and/or a component of subendocardial ischemia pattern). This is "shark fin" morphology. Code STEMI was activated. Eur Heart J.
This confirms that there were dynamic signs of ischemia on the initial ECG. In the interest of academic discussion — I’ll add the following thoughts: The computer interpretation was obviously wrong. Note that the ST elevation in the inferior leads has basically resolved, especially compared with the restored QRS voltage.
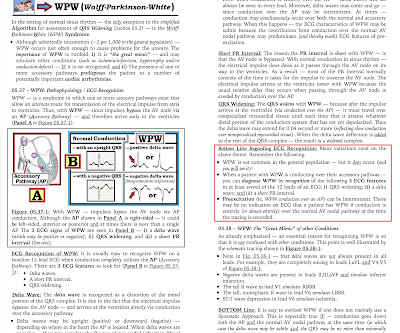
For the EP cardiologist — localization of the AP before EP study is more than academic, as it facilitates and expedites localization of the AP during EP study. ECG Blog #157 — Can you diagnose ischemia and/or infarction when there is WPW? ECG Blog #87 — Reviews a case of WPW with intermittent AP conduction.
PEARL #2 — Distinction between PMVT vs Torsades is more than academic. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. Acute ischemia? Both treatment and the response to therapy tends to be different with these 2 entities.
This is one case where it made a difference: Right Ventricular MI seen on ECG helps Angiographer to find Culprit Lesion Nevertheless, it is sometimes a fun academic exercise to try to predict the infarct artery: An elderly patient had onset of chest pain one hour prior. He called 911. Here is the prehospital ECG. What do you think?
The diagnosis typically requires classic clinical features, with no evidence of obstructive coronary disease, and typical findings of ischemia on functional studies. This happens. But its rare! A clinician with any grasp on reality would work up men, on average, more aggressively for coronary disease than women.
The amiodarone was discontinued and the patient did well. == MY Comment , by K EN G RAUER, MD ( 6/23 /2023 ): == From an academic standpoint — I love WCT ( W ide- C omplex T achycardia ) rhythms. Next day, the cardiologists were convinced (I think correctly) that this was SVT with aberrancy that was triggered by DKA.
Evidence of acute ischemia (may be subtle) vii. Academic Emergency Medicine., Academic Emergency Medicine, 2003 Volume 10, Number 5 539-540. ST segment and T wave abnormalities consistent with or possibly related to myocardial ischemia. 2nd or 3rd degree AV blocks or sinus pause of at least 2 seconds iv. Left BBB vi.
This case highlights how T-waves are very important in the assessment of ischemia and dynamic changes in acute coronary syndrome. I have often seen colleagues worry about T-wave inversions as a sign of ongoing ischemia. Academic Emergency Medicine 27(S1): S220; May 2020. See this case: A man his 50s with chest pain.
It is a strange academic habit among cardiologists, that they have subdivided medical management into optimal and suboptimal. Academic lessons from this patient. The therapeutics of coronary stenosis has become a technogical wonder, interwoven with statistical wordplay in the last few decades. 2016 Dec;9(12):e003726.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content