This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
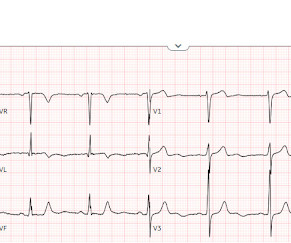
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands.
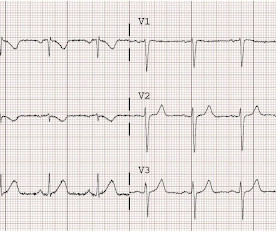
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chestpain that started 2-3 hours earlier while sitting on a porch swing. See this post: Septal STEMI with ST elevation in V1 and V4R, and reciprocal ST depression in V5, V6. Also seen in inferior + RV OMI.)
Written by Jesse McLaren Three patients presented with acute chestpain and ECGs that were labeled by the computer as completely normal, and which was confirmed by the final cardiology interpretation (which is blinded to patient outcome) also as completely normal. What do you think?
A 67 yo f developed chestpain this morning." Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. See this case: A man his 50s with chestpain.
A 50-something man presented in shock with severe chestpain. There is an obvious inferior posterior STEMI(+) OMI. We recorded an ECG in which V1-V3 were put in the position of V4R-V6R, and V4-6 were placed in V7-9 to (academically) confirm posterior OMI. His prehospital ECG was diagnostic of inferior posterior OMI.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Academic Emergency Medicine 27(S1): S220. Lupu L, et al. mg/dL, K 3.5
It is from a 50-something with chestpain: What do you think? This was marked as "Not a STEMI" by the physicians. It is not a STEMI, but it is diagnostic of an LAD OMI (Occlusion MI). has outperformed many cardiologists in its ability to recognize with "high confidence" acute OMIs from ECGs not satisfying STEMI-criteria.
He then went on to say: "40-something with chestpain for one hour. Burning pain subxiphoid and into throat." Still does not meet STEMI criteria, but it is an obvious OMI And then another one became more obvious: Cath lab was activated and a 100% RCA occlusion was found. Sounds like reflux, right? Learning Points: 1.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. See this case: A man his 50s with chestpain.
Written by Willy Frick A 50 year old man with no medical history presented with acute onset substernal chestpain. This was a machine read STEMI positive OMI. His ECG is shown below. Pretty obvious anterior current of injury. Readers of this blog can easily appreciate the hyperacute T waves in the precordium, clearest in V1-V4.
This is a 58 year old male with 40 minutes of chestpain of acute onset. He called 911 and paramedics recorded a prehospital 12 lead ECG which showed a clear inferior STEMI (not shown, tracing could not be found). He was given aspirin and sublingual nitroglycerine, which improved his pain. 18 (5 Suppl 1):Abstract 425, p.
Sent by anonymous, edited by Pendell Meyers A man in his 50s with history only of hypertension presented with acute chestpain that started 45 minutes prior to presentation while doing yard work. Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI").
This was sent by : Jacob Smith, DO Emergency Medicine Resident Ohio Health Doctors Hospital Emergency Residency Christopher Lloyd, DO, FACEP Director of Clinical Education, USACS Midwest Case A 30 year old patient presents to triage with chestpain. This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI."
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion.
Code STEMI was activated. What is the Diagnosis in this 70-something with ChestPain? 68 minutes with chest compressions, full recovery. A man in his 80s with chestpain What, besides large anterior STEMI, is so ominous about this ECG? The patient arrived to the ED in cardiogenic shock but awake.
Factors consistently manifesting as such, in addition to chestpain, include, diaphoresis, vomiting, radiation of pain (most alarming when inclusive of both arms), and pain aggravated by exertion. [1] It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS).
He has a history of coronary artery disease and a STEMI two years prior that was treated with primary PCI. He contacted EMS due to acute onset chestpain and feeling unwell and fatigued. He subsequently developed worsening chestpain. Pain is improving and ischemic T-wave inversions are no longer present".
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content