This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
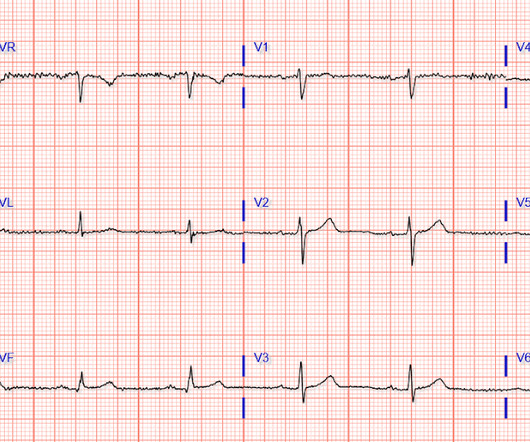
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chestpain that started 2-3 hours earlier while sitting on a porch swing. V1 sits over both the RV and the septum, so transmural ischemia of either one with give OMI pattern in V1 and reciprocal STD in V5 and V6.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Academic Emergency Medicine 27(S1): S220. Abstract 556.
He then went on to say: "40-something with chestpain for one hour. Burning pain subxiphoid and into throat." It does not usually represent subendocardial ischemia, but rather it is usually reciprocal ST depression, reciprocal to inferior ST elevation. Had episode of nausea and dizziness when it started.
Dr. Stone is Director of Academic Affairs for the Mount Sinai Health System and Professor of Medicine (Cardiology) and Professor of Population Health Science and Policy at the Icahn School of Medicine at Mount Sinai, and the study chair of the ECLIPSE trial. These results extend the strong recommendations from recent U.S.
A 67 yo f developed chestpain this morning." There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). See this case: A man his 50s with chestpain. Academic Emergency Medicine 27(S1): S220; May 2020.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. For now she can only say Not OMI.
Written by Willy Frick A 50 year old man with no medical history presented with acute onset substernal chestpain. In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. His ECG is shown below.
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). Here are some cases of RBBB with LAFB: What is the Diagnosis in this 70-something with ChestPain? There is STE in aVR.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Thanks for reading Dr. The data is overwhelming every way you can possibly look at it.
A middle-aged woman had an acute onset of chestpain and dyspnea. The pain had almost resolved by the time an ECG was obtained in the ED: Here is the computer diagnosis What do you think? This confirms that there were dynamic signs of ischemia on the initial ECG. The ST depression in aVL is also resolved.
The chestpain quickly subsided. Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. This distinction is more than academic — because both treatment and the response to therapy tend to be different with these 2 entities. Acute ischemia? Use of QT-prolonging drugs?
Traditional methods of non-invasive ischemia testing (stress EKG , stress echo, SPECT , PET , direct-to-cath) can result in false negatives 20-30 percent of the time, which can lead to undetected disease, and false positives over 50 percent of the time, which can lead to unnecessary invasive procedures. 2021 ACC/AHA ChestPain Guidelines.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. There is no definite evidence of acute ischemia. (ie, The below ECG was recorded.
The ECG is diagnostic of LAD occlusion (or even left main occlusion possibly), with the classic pattern of RBBB and LAFB with huge concordant STE in V1-V2, I, and aVL, with reciprocal depression in most other leads (and/or a component of subendocardial ischemia pattern). What is the Diagnosis in this 70-something with ChestPain?
Sent by anonymous, edited by Pendell Meyers A man in his 50s with history only of hypertension presented with acute chestpain that started 45 minutes prior to presentation while doing yard work. Smith : the profound persistent STE suggests either persistent occlusion or " no reflow " with persistent downstream ischemia.
This is one case where it made a difference: Right Ventricular MI seen on ECG helps Angiographer to find Culprit Lesion Nevertheless, it is sometimes a fun academic exercise to try to predict the infarct artery: An elderly patient had onset of chestpain one hour prior. He called 911. Here is the prehospital ECG.
A recent similar case: A 40-something with chestpain. PEARL #2 — Distinction between PMVT vs Torsades is more than academic. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. Acute ischemia? Is this inferior MI?
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Evidence of acute ischemia (may be subtle) vii. Academic Emergency Medicine.,
He contacted EMS due to acute onset chestpain and feeling unwell and fatigued. He subsequently developed worsening chestpain. This, in the context of worsening chestpain , is evidence of reocclusion of the infarct-related artery and active OMI in development. The below ECG was recorded. What do you think?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content