This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
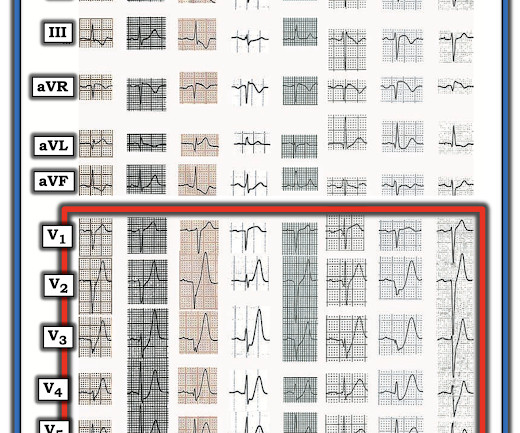
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia.
This is one case where it made a difference: Right Ventricular MI seen on ECG helps Angiographer to find Culprit Lesion Nevertheless, it is sometimes a fun academic exercise to try to predict the infarct artery: An elderly patient had onset of chest pain one hour prior. His included cardiogenicshock, V Tach, AV block.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenicshock" is not applicable outside of sinus rhythm. In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished.
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). Today's patient did make it to the hospital — but was in cardiogenicshock, and despite valiant attempt at treatment, succumbed soon after.
The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. There is no definite evidence of acute ischemia. (ie, Distinction of PMVT vs VFib is an academic one in this case ). Some residual ischemia in the infarct border might still be present.
The ECG is diagnostic of LAD occlusion (or even left main occlusion possibly), with the classic pattern of RBBB and LAFB with huge concordant STE in V1-V2, I, and aVL, with reciprocal depression in most other leads (and/or a component of subendocardial ischemia pattern). The patient arrived to the ED in cardiogenicshock but awake.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content