This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
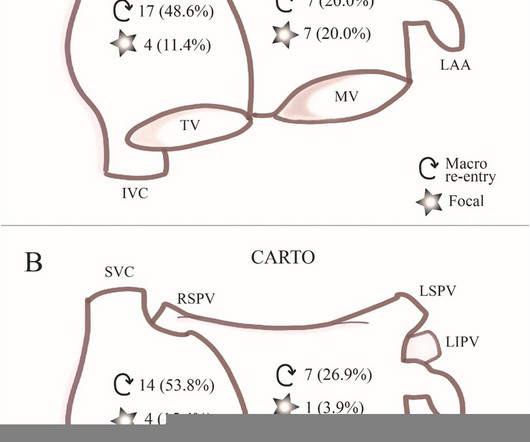
Distribution Variance of Focal Atrial Tachycardia Foci and Long-Term Outcomes After Ablation. ABSTRACT Introduction The distribution of the origin of focal atrial tachycardia (FAT) in patients with different ages have not been clearly elucidated. After a mean follow-up of 47.2 months, FAT recurred in 57 patients.
Among patients with ventricular tachycardia and ischemic cardiomyopathy, catheter ablation as an initial therapy led to a lower risk of adverse outcomes than antiarrhythmic drug therapy.
Cingolani, director of Cardiogenetics and Preclinical Research in the Department of Cardiology in the Smidt Heart Institute at Cedars-Sinai, is exploring new ways to help patients with ventricular tachycardia (VT), a recurring, abnormally fast and irregular heartbeat that starts in the lower chambers, or ventricles, of the heart.
The goal of the VANISH2 trial was to compare endocardial catheter ablation with conventional antiarrhythmic drug (AAD) therapy as a first-line treatment for infarct-related ventricular tachycardia (VT) in ischemic cardiomyopathy.
A multicenter study has described and validated a new strategy for guiding ablation procedures in patients with complex tachycardias. Ablation procedures use energy—usually heat or cold—to eliminate small areas of heart tissue that cause pathological cardiac arrhythmias, thereby restoring normal heart rhythm.
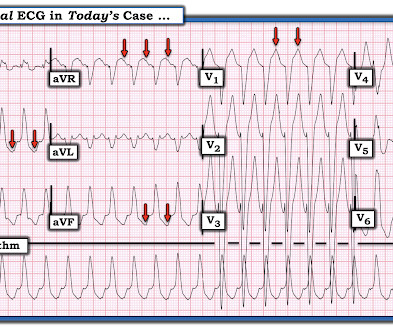
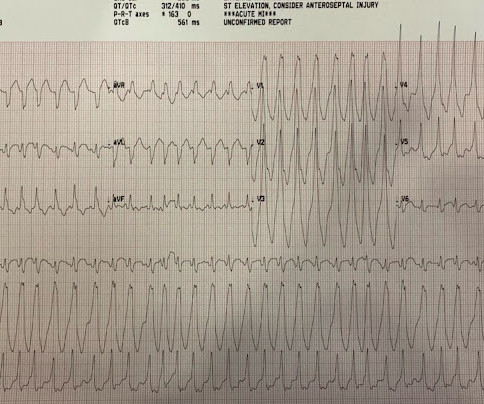
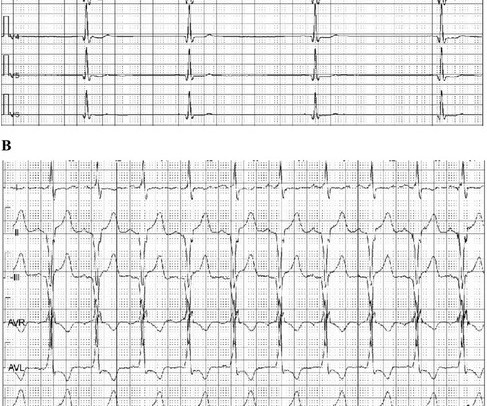
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
BACKGROUND:Current outcomes from catheter ablation for scar-dependent ventricular tachycardia (VT) are limited by high recurrence rates and long procedure durations. Predicted optimum ablation sites to terminate all VTs in the models were identified. Rapid-pacing protocols were used to induce VTs and to define the VT circuits.
Electroanatomic mapping guides complex atrial tachycardiaablations; however, challenges may emerge after pulmonary vein isolation. 3D mapping systems can reveal the mechanism of tachycardia and critical areas that need to be ablated.
The ECGs show a wide complex, irregularly irregular tachycardia. An accessory pathway was identified and was ablated. The patient has not had any recurrent episodes of atrial fibrillation and has a narrow QRS complex without delta wave on his ECG post ablation. So he was simply discharged without EP study.
Outcomes of ablation with the FARAPULSE PFA System – a nonthermal treatment in which electric fields selectively ablate heart tissue – will be compared to outcomes following use of anti-arrhythmic drug (AAD) therapy, which is commonly prescribed for patients living with persistent AF. The company now anticipates U.S. Circulation.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
Five criteria predict whether patients are likely or unlikely to have supraventricular tachycardia induced or ablated at an electrophysiologic study (EPS). Methods We performed a retrospective chart review of 1089 patients referred for EPS and ablation of SVT at 2 high volume centers. 001; Ablation, 88% versus 26%, RR = 3.32 (2.48–4.46),
What are the outcomes of patients referred for ventricular tachycardia (VT) ablation according to left ventricular ejection fraction (LVEF), tolerance of VT, and acute ablation outcome?
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation.
The first randomized trial to investigate preventive ablation of a potential arrhythmogenic substrate associated with coronary chronic total occlusion (CTO) in patients at high risk of ventricular arrhythmias (VAs) reduces the risk of appropriate implantable cardioverter-defibrillator (ICD) therapy and unplanned hospitalization in patients with no (..)
Abstract Introduction Understanding the spatiotemporal location of the spontaneous termination of ventricular tachycardia (VT) may provide new insights for ablation. These findings may help guide future studies into improving the success of VT ablation.
But it is not disorganized enough to be polymorphic ventricular tachycardia. The patient did well and was referred for ablation. Learning Points: Wide complex irregularly irregular tachycardias include PMVT, AF with WPW, and AF with aberrancy. See our other cases of AF with WPW: A young man with another episode of tachycardia.
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. On the ECG, ventricular tachycardia can be defined as three or more ventricular ectopic beats occurring in a sequence at a rate more than 100 per minute. Another rare form of ventricular tachycardia is bidirectional ventricular tachycardia.
Using ECG recording and deductive reasoning, our teachers and predecessors classified the bradycardias and tachycardias and proposed many mechanisms, subsequently proven to be correct. Notwithstanding many insightful observations, the electrocardiogram (ECG) arguably ignited the big bang in our understanding of cardiac arrhythmias.
The goals of the current scientific research on ventricular tachycardia (VT) ablation included studies to prove the benefit of early ablation on heart failure progression and mortality and the need to better characterize and treat heterogeneous deep VT substrates.
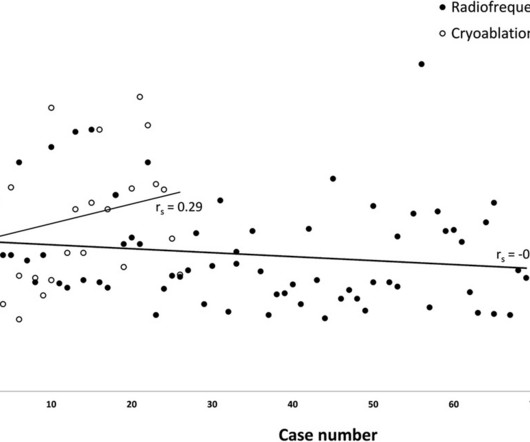
BackgroundCryoablation for pediatric atrioventricular nodal reentry tachycardia (AVNRT) is favored for reducing conduction system injury compared to radiofrequency (RF) ablation. ResultsAmong 95 patients, 69 received RF ablation and 26 received cryoablation. Recurrence rates were 2.9% vs. 11.5%, p>0.99).
Catheter ablation as a treatment for ventricular tachycardia has lagged behind ablation procedures for atrial arrhythmias in becoming an established first-line therapy.
IntroductionAtrial tachycardia (AT) frequently occurs after cardiac surgery or surgical ablation procedures. The novel charge density-based mapping system (CDM) provides global chamber mapping and can detect crucial pathways of conduction; therefore, it has potential added value in catheter ablation (CA) of post-surgical ATs.
Typically, patients with HCM experience sinus tachycardia and sinus arrest relatively infrequently. Meanwhile, a dual-chamber pacemaker can treat HCM by changing the sequence of myocardial contraction.
Personalized heart digital twin models accurately detect substrate and functional abnormalities during ablation for scar-dependent ventricular tachycardia (VT).
The best approach for ablating ventricular tachycardia (VT) targeting right ventricular free wall (RVFW) aneurysms in arrhythmogenic right ventricular cardiomyopathy (ARVC) remains undefined.
Abstract Introduction Some previous studies have reported that a first-step ethanol infusion into the vein of Marshall (EIVOM) with touch-up radiofrequency (RF) ablation can facilitate mitral isthmus (MI) block and improves the ablation outcomes in persistent atrial fibrillation (PeAF) patients. 0.78, p = .006).
Pericarditis is the most common complication following hybrid sinus node sparing ablation for Inappropriate Sinus Tachycardia (IST)/Postural Orthostatic Tachycardia Syndrome (POTS).
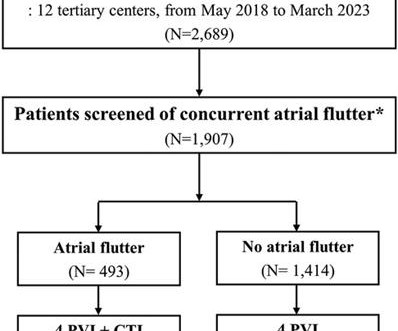
This study investigated the association between concurrent typical atrial flutter and cavotricuspid isthmus (CTI) ablation and the recurrence of atrial arrhythmia. The data were obtained from a multicenter registry of cryoballoon ablation for AF ( n = 2,689). All the patients with typical atrial flutter underwent CTI ablation.
A novel sinus node (SN) sparing hybrid ablation for inappropriate sinus node tachycardia (IST)/Postural Orthostatic Tachycardia Syndrome (POTS) has been demonstrated to be an effective and safe therapeutic option in patients with symptomatic drug-resistant IST/POTS.
Initial catheter ablation achieved a lower risk of a composite primary endpoint event than anti-arrhythmic drug therapy in patients who survived a heart attack.
Among patients with ischemic cardiomyopathy and ventricular tachycardia (VT), catheter ablation as a first-line strategy over antiarrhythmic drugs (AAD) was associated with a lower risk of the primary outcome, according to results of the VANISH2 trial.
Biatrial atrial tachycardia (BiAT) is a rare form of atypical macro-reentrant AT (MRAT) that can be difficult to characterize and ablate. Ablation of regions demonstrating spatiotemporal dispersion (SD) has shown a high rate of atrial fibrillation (AF) termination to either sinus or MRAT during ablation.
Ablation of regions demonstrating spatiotemporal dispersion (SD) has been demonstrated as an alternative strategy beyond pulmonary vein isolation in patients with persistent atrial fibrillation. Occurrence of atrial tachycardia (AT) following ablation remains a limitation of this approach.
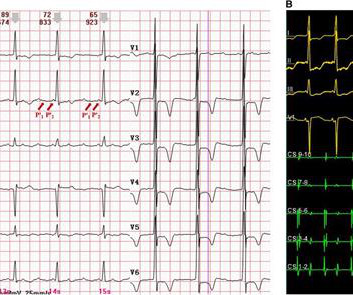
However, widely split P' waves in focal atrial tachycardia (AT) on a surface electrocardiogram (ECG) have rarely been reported. Case summary A 67-year-old patient, who had undergone two radiofrequency ablations for atrial fibrillation, presented with recurrent palpitation.
Catheter ablation is an effective therapy for ventricular tachycardia (VT) and is increasing in use. Assessment of contemporary real-world outcomes of VT ablation requires data inclusive of both inpatient and outpatient encounters.
What is the feasibility and safety of ventricular tachycardia (VT) ablation in patients with structural heart disease using a zero-fluoroscopy approach?
Atrioventricular Nodal Reentrant Tachycardia (AVNRT) represents the most frequent, regular tachyarrhythmia in humans, but its exact circuit has so far remained elusive.
She had previously undergone three prior endocardial radiofrequency ablations for scar-related ventricular tachycardia (VT) with the most recent procedure at our center 4 months prior to the current hospital presentation.
Recurrent ventricular tachycardia (VT) can be treated by substrate modification of the myocardial scar by catheter ablation during sinus rhythm without VT induction. Better defining this arrhythmic substrate could help improve outcome and reduce ablation burden.
IntroductionFocal atrial tachycardia (FAT) is predominant in the pediatric population. A 12-lead electrocardiogram revealed a narrow QRS complex tachycardia with a rate of 157 beats per minute and a prolonged RP relationship. Echocardiography indicated a severely reduced ejection fraction of 22%.
Twenty‐six PVT/ventricular fibrillation–triggering PVCs were identified for ablation. After a mean follow‐up of 49 months after ablation, 8 (57%) patients were free from syncope recurrence. Ablation of trigger beat significantly reduced the syncope frequency (mean±SD, 4.3±1.6
Catheter-ablation (CA) of consecutive left atrial tachycardias (LAT) can be challenging. So far, pulsed field ablation (PFA) has not been compared to radiofrequency current (RFC) energy in CA of LAT.
Patients with inappropriate sinus tachycardia (IST) have a significant change in quality of life and are unable to tolerate medications due to side effects. Recently sinus node sparing hybrid ablation (that includes endocardial right atrial ablation and video assisted thoracoscopic epicardial surgical (VATS) ablation) has been described.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content