This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
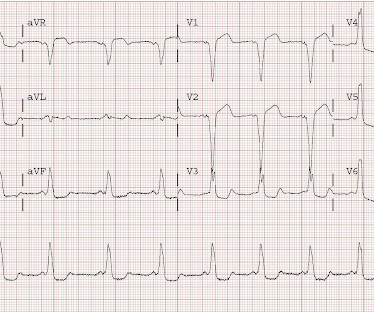
One might think this represents acute STEMI, or Bundle branch block with discordant ST segments and suspicously concordant T-waves. Ablation was planned for a later date. Upon arrival to the ED, he had the following 12-lead ECG: There is striking ST segment elevation in V1 and V2, with ST depression in V3-V6 as well as I, II, and aVF.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. In such cases — radiofrequency ablation of ectopic beats triggering malignant ventricular arrhythmias was needed for control of arrhythmic storm because the antiarrhythmic medications tried were ineffective ( Marrouche et al — JACC 5;43(9): 1715-20, 2004 ).
In other words, after reperfusion therapy for STEMI, the appearance of AIVR is usually a good sign, meaning that the artery is reperfused. Our electrophysiologist, Rehan Karim, states he has ablated AVNR"T" ("T" because it is not tachycardia) in a 90 year old, and that he has seen rate-related BBB at very slow rates.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chest pain and SOB. Thus, Wellens' syndrome should be thought of as a transient OMI or transient STEMI. Transient STEMI is at high risk of re-occlusion. This was sent by a colleague.
But it doesn’t meet STEMI criteria, and was not identified by the computer or the over-reading cardiologist. Still no WPW pattern, and more obvious inferoposterior OMI, but still STEMI negative. The emergency physician wasn’t sure what to make of the changes from one ECG to the next but was concerned about ACS. What do you think?
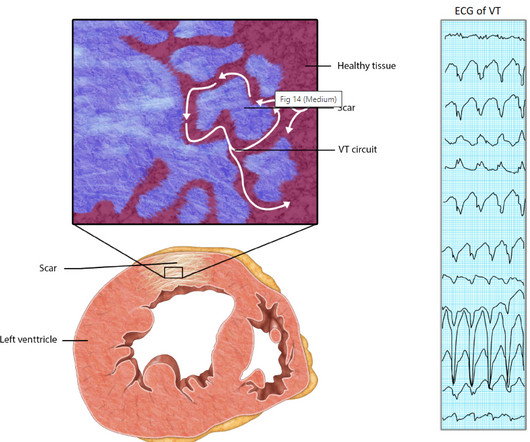
There is a problem here too ,even critical Ischemia with high grade unstable angina rarely trigger a VT but STEMI seems to have the exclusive rights to trigger it , by its ability to produce acute transmural ischemia. best , it is just a back up device to tackle the escaped VTs in spite of RF ablation and drugs. Reference 1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content