This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Distribution Variance of Focal Atrial Tachycardia Foci and Long-Term Outcomes After Ablation. ABSTRACT Introduction The distribution of the origin of focal atrial tachycardia (FAT) in patients with different ages have not been clearly elucidated. After a mean follow-up of 47.2 months, FAT recurred in 57 patients.
Electroanatomic mapping guides complex atrial tachycardiaablations; however, challenges may emerge after pulmonary vein isolation. 3D mapping systems can reveal the mechanism of tachycardia and critical areas that need to be ablated.
Outcomes of ablation with the FARAPULSE PFA System – a nonthermal treatment in which electric fields selectively ablate heart tissue – will be compared to outcomes following use of anti-arrhythmic drug (AAD) therapy, which is commonly prescribed for patients living with persistent AF. The company now anticipates U.S. Circulation.
Abstract Introduction Some previous studies have reported that a first-step ethanol infusion into the vein of Marshall (EIVOM) with touch-up radiofrequency (RF) ablation can facilitate mitral isthmus (MI) block and improves the ablation outcomes in persistent atrial fibrillation (PeAF) patients. 0.78, p = .006).
Ablation of regions demonstrating spatiotemporal dispersion (SD) has been demonstrated as an alternative strategy beyond pulmonary vein isolation in patients with persistent atrial fibrillation. Occurrence of atrial tachycardia (AT) following ablation remains a limitation of this approach.
Epicardial Marshall bundle (MB) are frequently utilized in left atrial tachycardias (LATs) post atrial fibrillation (AF) ablation with pulmonary vein isolation and substrate modification.
A 77-year-old male with a history of two catheter ablation procedures, including pulmonary vein isolation and superior vena cava (SVC) isolation, presented with symptomatic palpitations. A twelve-lead electrocardiogram revealed atrial tachycardia (AT) with a cycle length of 240 ms.
Both atria develop from a combination of the primitive atrium, sinus venous, and pulmonary veins.It In all probability, this dilation is a form of atrial tachycardia and atrial cardiomyopathy. In contrast to other tachycardias, with atrial fibrillation (AF), the focus is often speculative, and ablation attempts are made accordingly.
Pulse field ablation (PFA) using a pentaspline catheter is an effective and safe treatment method for pulmonary vein isolation (PVI) in patients with atrial fibrillation (AF).1,2 We present a case of a macro-reentrant atrial tachycardia in the lateral right atrium (RA) treated by PFA using a pentaspline catheter.
The combined solutions are expected to enhance performance and streamline workflows for electrophysiologists during catheter ablation procedures to treat atrial fibrillation , AFib. Secondary endpoints include absence of AF and/or atrial tachycardia (AT) episodes after a 12-month period, following one or more procedures, as well as safety.
ABSTRACT Background Real-life data on efficacy and safety of pulsed-field ablation (PFA) using the pentaspline multi-electrode catheter in symptomatic atrial fibrillation (AF) patients is still scarce. Objective This study aims to assess the efficacy and safety of PFA in patients with persistent AF. Major complications occurred in 2.0%
Pulsed-field ablation (PFA) is becoming increasingly relevant in the field of electrophysiology. Besides single-shot PFA devices for pulmonary vein isolation (PVI), point-by-point PFA is also gaining importance due to many possible applications. Data on the use is sparse, especially for atrial tachycardia (AT).
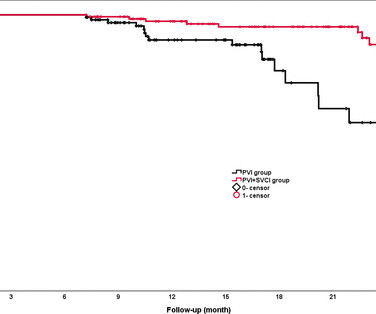
Background The value of empirical superior vena cava isolation (SVCI) following pulmonary vein isolation (PVI) to improve the efficacy of radiofrequency catheter ablation (RFCA) for paroxysmal atrial fibrillation (PAF) remains controversial. RFCA was guided by quantitative AI in both groups. vs 81.5%, p=0.02). 95% CI 0.19
Backgroundwide antral pulmonary vein isolation (PVI) is effective for treating paroxysmal atrial fibrillation (PAF), although time-demanding. Procedural data and electrophysiology (EP) laboratory times were systematically collected and analyzed.
Extra-pulmonary vein (PV) triggers have been reported in up to 4.9-15% 15% of all atrial fibrillation (AF) patients who undergo catheter ablation and plays significant roles in arrhythmia recurrence.1,2 Extra-pulmonary vein (PV) triggers have been reported in up to 4.9-15%
Pulsed field ablation (PFA) has become increasingly important in the treatment of cardiac arrhythmias. In addition to single-shot devices mainly used for pulmonary vein isolation, focal PFA may provide a treatment option that increases the versatility of the technique.
Vein of Marshall ethanol ablation (VOM-EA) as an adjunct to pulmonary vein isolation (PVI) has been reported to improve freedom from atrial fibrillation (AF) and atrial tachycardia (AT).
Abstract Background The newly introduced nonthermal pulsed field ablation (PFA) is a promising technology to achieve fast pulmonary vein isolation (PVI) with high acute success rates and good safety features. Data comparing PFA to VHPSD-PVI is lacking. Two tamponades occurred in the PFA while in VHPSD two pts suffered groin bleedings.
a global leader in cardiac arrhythmia treatment and part of Johnson & Johnson MedTech , today announced European CE mark approval of the VARIPULSE Platform for the treatment of symptomatic drug refractory recurrent paroxysmal atrial fibrillation ( AF ) using pulsed field ablation (PFA). iii] The study reported a low fluoroscopy time of 7.8
Particularly in cases of repaired tetralogy of Fallot or double-outlet right ventricle (DORV), a scar resulting from surgery at the right ventricular outflow tract (RVOT) is one of the factors for ventricular tachycardias (VTs).
Methods and Results This case report discusses a 65-year-old man who had previously undergone pulmonary vein isolation (PVI) and cavo-tricuspid isthmus ablation for atrial fibrillation before ASD closure, respectively. He developed atrial tachycardia (AT) and underwent catheter ablation.
Pulsed field ablation (PFA) may overcome the disadvantages of thermal energy and improve both ablation efficacy and safety. Coronary vasospasm occurred (and quickly resolved after injection of nitroglycerin) in one patient during additional ablation of a focal atrial tachycardia at the coronary sinus ostium.
FAAM ablation successfully decreased the recurrence rate of atrial tachyarrhythmia compared with conventional non-PV foci ablation. Abstract Introduction Treatment of recurrent atrial fibrillation (AF) is sometimes challenging due to non-pulmonary vein (PV) foci. The RHYTHMIA system was used to perform all the procedures.
Abstract The QDOT MICRO™ Catheter is a novel open-irrigated contact force-sensing radiofrequency ablation catheter. It offers very high-power short-duration (vHPSD) ablation with 90 W for 4 s to improve safety and efficacy of catheter ablation procedures.
Abstract Introduction It would be helpful in determining ablation strategy if the occurrence of perimitral atrial tachycardia (PMAT) could be predicted in advance. Conclusion Short E-PMCT may predict noninducibility of PMAT and guide a less invasive ablation strategy. We calculated their E-PMCT.
Commonly employed empiric strategies for catheter ablation (CA) of refractory atrial fibrillation (AF) beyond pulmonary vein isolation (PVI) include posterior wall isolation (PWI), linear ablation involving left atrial (LA) roof and mitral lines, as well as targeting of areas of low voltage / myopathy.
Abstract Introduction Despite advanced ablation strategies and major technological improvements, treatment of persistent atrial fibrillation (AF) remains challenging and the underlying pathophysiology is not fully understood. ms after) and AF termination to atrial tachycardia (AT) or sinus rhythm (SR) in 12 patients (24%).
Over the past years, patients with tetralogy of Fallot (TOF) have experienced numerous improvements in different treatment modalities consisting of a mixture of surgical procedures, transcatheter interventions including ablation therapy, and implantable cardioverter-defibrillator implantation procedures.
A 37-year-old woman with biventricular repair for pulmonary atresia and an intact ventricular septum was referred for an electrophysiological study in the context of recurrent atrial arrhythmias with multiple electrical cardioversions. Her clinical tachycardia was easily inducible and had a cycle length (TCL) of 340 ms.
The cyanosis in Ebstein’s anomaly, is usually not due to pulmonary hypertension, but because tricuspid regurgitation jet is directed across the atrial septal defect. Electrophysiological study will show that, and this pathway can be ablated. This is one important cause of supraventricular tachycardia in Ebstein’s anomaly.
Crochetage sign on ECG in ASD ECG in ASD with severe pulmonary hypertension: Tall R’ in V1, ST depression in inferior leads and V2-V5, and T inversion in inferior leads and V1-V6 are seen. Multiple accessory pathways can occur and radiofrequency catheter ablation is effective.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chest pain and SOB. No signs for aortic dissection or pulmonary embolus. --"Results were discussed with the ordering physician. This was sent by a colleague. Deep breaths are painful and symptoms come and go.
Further ultrasound showed no B-lines (no pulmonary edema). Unless there is a dramatic response to being put back on beta-blocker therapy — consideration of S eptal R eduction T herapy ( SRT ) , in the form of either surgical myomectomy or alcohol septal ablation, performed at a center with experience in this area may soon be needed.
Background:Patients with adult congenital heart disease (ACHD) form a unique subset of patients with complex ventricular tachycardia (VT).Objective:To The primary composite outcome was recurrent monomorphic VT, and repeat ablation.Results:Out of 508 procedures for ventricular tachycardiaablation, 37 were performed in ACHD patients.
ABSTRACT Background Catheter ablation (CA) for atrial fibrillation (AF) in the elderly poses a growing challenge. Methods Octogenarians with AF or consecutive atrial tachycardia undergoing index or re-ablation (pulmonary vein isolation [PVI] and ablation beyond PVI with different energy sources) in a single center, were analyzed.
BACKGROUND:Patients undergoing first-time atrial fibrillation (AF) ablation can benefit from targeting non-pulmonary vein (PV) triggers. Preprocedural identification of high-risk individuals can guide planning of ablation strategy. Among all first-time AF ablations, 68.1% were intermediate-risk (score 2, 10.5%
Abstract Introduction Pulsed field ablation (PFA) is a new ablation technology for atrial fibrillation (AF). Data regarding early recurrences of atrial tachyarrhythmia (ERAT) after PFA-pulmonary vein isolation (PVI) are sparse. We found no difference in the rate of LRs among patients experiencing ERAT before or after 45 days.
ABSTRACT Introduction The safety and efficacy of paroxysmal atrial fibrillation (PAF) ablation with the HELIOSTAR multielectrode radiofrequency (RF) balloon catheter have been demonstrated in European studies; data from elsewhere are lacking. The primary safety endpoint was the occurrence of early-onset primary adverse events (PAEs).
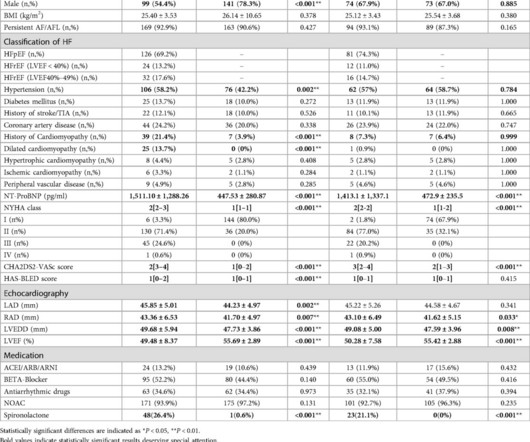
Currently, ethanol infusion of vein of Marshall (EIVOM) for AF ablation in HF patients remains significantly limited.MethodThis was a non-randomized, single-center, retrospective observational study. AF patients received 4-step ablation composed of EIVOM, pulmonary vein isolation (PVI) and linear ablation.
For right or wrong reasons, the world of electrophysiology has pushed us into a belief system that, if it is AF, the culprit must be pulmonary veins. In fact, non-pulmonary vein origins can be a staggering 70% in some series. If we look at the above map,RA prevails over LA convincigly in termes of focal atrial tachycardia.
ABSTRACT Introduction Freedom from recurrences of atrial tachyarrhythmia (ATA) is suboptimal after pulmonary vein isolation (PVI) in patients with persistent atrial fibrillation (PsAF). This sub-analysis from the Cryo Global Registry sought to investigate predictors of ablation success after PVI using cryoballoon ablation (CBA) for PsAF.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content